Jeong Hun Seo, Kwang Jin Chun, Bong-Ki Lee, Byung-Ryul Cho, Dong Ryeol Ryu
{"title":"Aortic valve sclerosis is not a benign finding but progressive disease associated with poor cardiovascular outcomes.","authors":"Jeong Hun Seo, Kwang Jin Chun, Bong-Ki Lee, Byung-Ryul Cho, Dong Ryeol Ryu","doi":"10.1186/s44348-024-00037-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aortic valve sclerosis (AVS) shares risk factors with atherosclerosis. However, the relationship between AVS progression with cardiovascular (CV) risk has not been researched. This study investigates CV outcomes according to progression of AVS.</p><p><strong>Methods: </strong>This study included 2,901 patients with AVS (irregular leaflet thickening and peak aortic jet velocity < 2 m/sec) who underwent serial echocardiograms at least 1 year apart during 2011-2020. The primary outcome was defined as CV death, myocardial infarction, stroke, or revascularization.</p><p><strong>Results: </strong>During a median follow-up period of 3.9 years, 439 of 2,901 AVS patients (15.1%) progressed to mild or greater aortic stenosis. Patients with progression were older and more likely to have atrial fibrillation than those without. In a stepwise regression, age (odds ratio [OR] per 1-year increase, 1.04; 95% confidence interval [CI], 1.01-1.07), peripheral artery disease (OR, 9.07; 95% CI, 3.12-26.4), and left ventricular mass index (OR per 1-g/m<sup>2</sup> increase, 1.01; 95% CI, 1.00-1.02) were associated with AVS progression. Over a median of 6.3 years, the primary outcome occurred in 858 of 2,901 patients (29.6%). Patients with progression had higher frequency of CV death, myocardial infarction, stroke, or revascularization than those without progression (P < 0.0001). In Cox proportional hazards regression, AVS progression (hazard ratio, 1.33; 95% CI, 1.10-1.61) was a significant determinant of CV mortality.</p><p><strong>Conclusions: </strong>The progression to aortic stenosis in AVS patients is an independent risk factor for CV mortality. These findings suggest that patients with AVS progression may benefit from stricter CV risk monitoring.</p>","PeriodicalId":15229,"journal":{"name":"Journal of Cardiovascular Imaging","volume":"32 1","pages":"39"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11590455/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44348-024-00037-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Aortic valve sclerosis (AVS) shares risk factors with atherosclerosis. However, the relationship between AVS progression with cardiovascular (CV) risk has not been researched. This study investigates CV outcomes according to progression of AVS.
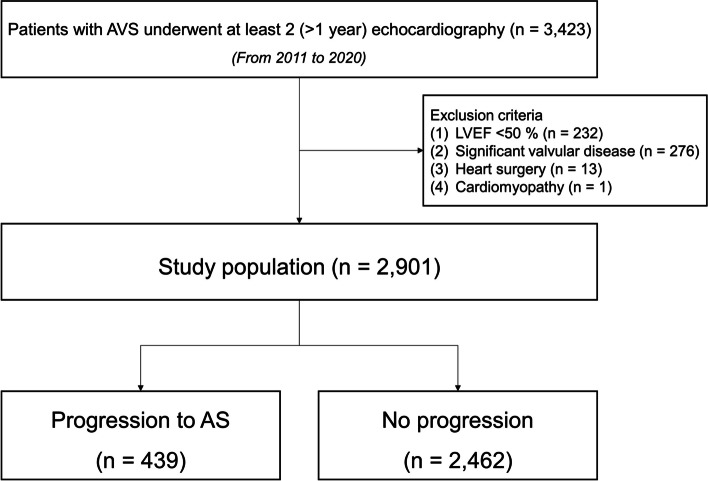
Methods: This study included 2,901 patients with AVS (irregular leaflet thickening and peak aortic jet velocity < 2 m/sec) who underwent serial echocardiograms at least 1 year apart during 2011-2020. The primary outcome was defined as CV death, myocardial infarction, stroke, or revascularization.
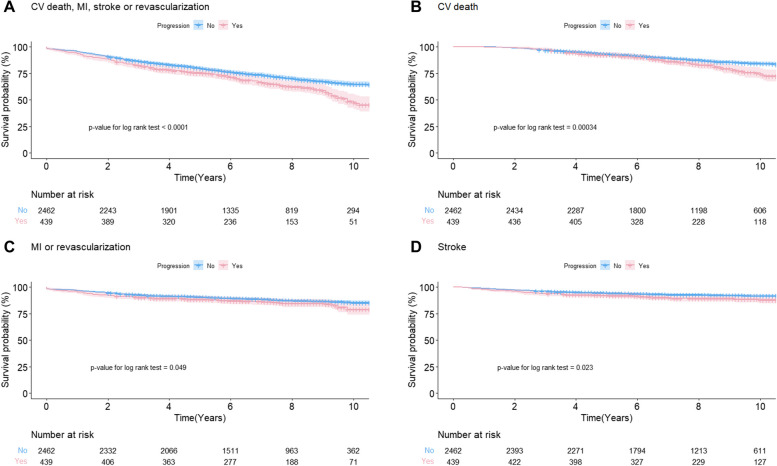
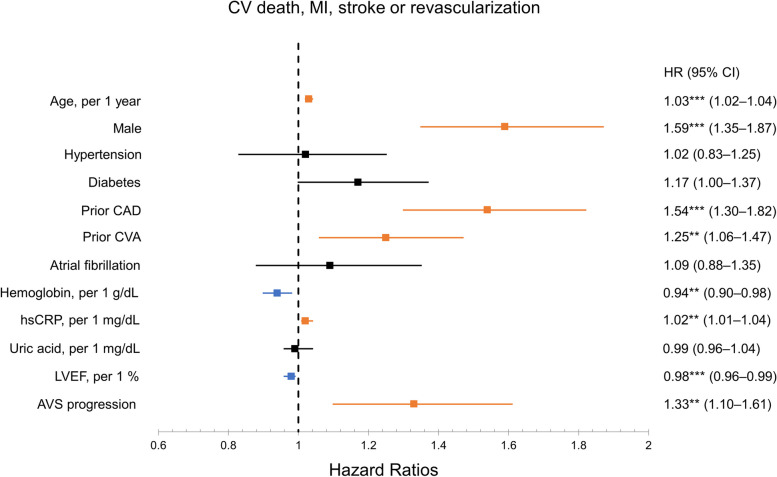
Results: During a median follow-up period of 3.9 years, 439 of 2,901 AVS patients (15.1%) progressed to mild or greater aortic stenosis. Patients with progression were older and more likely to have atrial fibrillation than those without. In a stepwise regression, age (odds ratio [OR] per 1-year increase, 1.04; 95% confidence interval [CI], 1.01-1.07), peripheral artery disease (OR, 9.07; 95% CI, 3.12-26.4), and left ventricular mass index (OR per 1-g/m2 increase, 1.01; 95% CI, 1.00-1.02) were associated with AVS progression. Over a median of 6.3 years, the primary outcome occurred in 858 of 2,901 patients (29.6%). Patients with progression had higher frequency of CV death, myocardial infarction, stroke, or revascularization than those without progression (P < 0.0001). In Cox proportional hazards regression, AVS progression (hazard ratio, 1.33; 95% CI, 1.10-1.61) was a significant determinant of CV mortality.
Conclusions: The progression to aortic stenosis in AVS patients is an independent risk factor for CV mortality. These findings suggest that patients with AVS progression may benefit from stricter CV risk monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


