Riccardo Ray Colciago, Chiara Chissotti, Federica Ferrario, Maria Belmonte, Giorgio Purrello, Valeria Faccenda, Denis Panizza, Stefania Canova, Gaia Passarella, Diego Luigi Cortinovis, Stefano Arcangeli
{"title":"Time to Next Treatment Following Sub-Ablative Progression Directed Radiation Therapy for Oligoprogressive Non-Small-Cell Lung Cancer.","authors":"Riccardo Ray Colciago, Chiara Chissotti, Federica Ferrario, Maria Belmonte, Giorgio Purrello, Valeria Faccenda, Denis Panizza, Stefania Canova, Gaia Passarella, Diego Luigi Cortinovis, Stefano Arcangeli","doi":"10.3390/curroncol31110505","DOIUrl":null,"url":null,"abstract":"<p><p>We aimed to evaluate whether progression-directed radiation therapy (PDRT) can prolong the initiation of a subsequent systemic therapy regimen in a cohort of patients with oligoprogressive NSCLC. A retrospective analysis was conducted on NSCLC patients who underwent PDRT for extracranial oligoprogressive NSCLC, defined as limited (up to five) progressing lesions following initial complete, partial, or stable response to systemic therapy according to REC1ST 1.1 and/or PERCIST 1.0 criteria. Cox proportional hazard regressions were performed to identify factors influencing time to next treatment (TTNT), which was considered the primary endpoint. Forty patients were analyzed. First, second, and ≥3 lines of systemic therapy were administered in 22 (58.2%), 14 (27.2%), and 4 (14.6%) cases, respectively. The median total dose was 36 Gy (range: 12-60) in five fractions (1-10), with a median biological effective dose for tumor control (BED10) of 52 Gy (26.4-151.2). After a median follow-up of 11 months (2-50), PDRT delayed further systemic therapy in 32 (80.0%) treatments. Median TTNT was not reached at 8 months (1-47) with a one-year Kaplan-Meier estimate of 81.4% (95% CI: 75.0% to 87.8%). No >grade 3 adverse event was observed. On multivariate analysis, patients with ≥3 lines of systemic therapy and/or with larger CTV volumes did not benefit from PDRT. Despite the use of sub-ablative doses, our findings show that PDRT represents an effective, safe, and viable option for oligoprogressive NSCLC. Patients irradiated early during their systemic treatment course, with a low volume of disease and nonmetastatic oligoprogression, could derive substantial benefits from PDRT.</p>","PeriodicalId":11012,"journal":{"name":"Current oncology","volume":"31 11","pages":"6840-6852"},"PeriodicalIF":3.4000,"publicationDate":"2024-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11592685/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/curroncol31110505","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
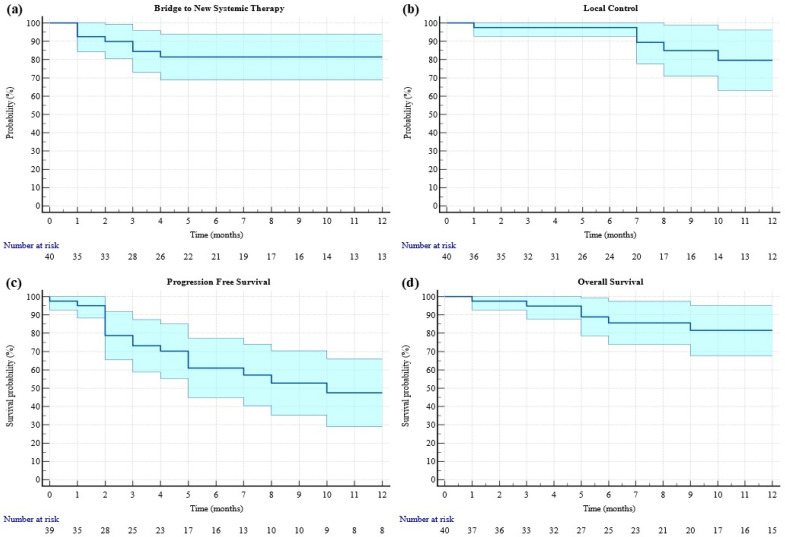
We aimed to evaluate whether progression-directed radiation therapy (PDRT) can prolong the initiation of a subsequent systemic therapy regimen in a cohort of patients with oligoprogressive NSCLC. A retrospective analysis was conducted on NSCLC patients who underwent PDRT for extracranial oligoprogressive NSCLC, defined as limited (up to five) progressing lesions following initial complete, partial, or stable response to systemic therapy according to REC1ST 1.1 and/or PERCIST 1.0 criteria. Cox proportional hazard regressions were performed to identify factors influencing time to next treatment (TTNT), which was considered the primary endpoint. Forty patients were analyzed. First, second, and ≥3 lines of systemic therapy were administered in 22 (58.2%), 14 (27.2%), and 4 (14.6%) cases, respectively. The median total dose was 36 Gy (range: 12-60) in five fractions (1-10), with a median biological effective dose for tumor control (BED10) of 52 Gy (26.4-151.2). After a median follow-up of 11 months (2-50), PDRT delayed further systemic therapy in 32 (80.0%) treatments. Median TTNT was not reached at 8 months (1-47) with a one-year Kaplan-Meier estimate of 81.4% (95% CI: 75.0% to 87.8%). No >grade 3 adverse event was observed. On multivariate analysis, patients with ≥3 lines of systemic therapy and/or with larger CTV volumes did not benefit from PDRT. Despite the use of sub-ablative doses, our findings show that PDRT represents an effective, safe, and viable option for oligoprogressive NSCLC. Patients irradiated early during their systemic treatment course, with a low volume of disease and nonmetastatic oligoprogression, could derive substantial benefits from PDRT.
期刊介绍:
Current Oncology is a peer-reviewed, Canadian-based and internationally respected journal. Current Oncology represents a multidisciplinary medium encompassing health care workers in the field of cancer therapy in Canada to report upon and to review progress in the management of this disease.
We encourage submissions from all fields of cancer medicine, including radiation oncology, surgical oncology, medical oncology, pediatric oncology, pathology, and cancer rehabilitation and survivorship. Articles published in the journal typically contain information that is relevant directly to clinical oncology practice, and have clear potential for application to the current or future practice of cancer medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


