Natalie J Chandler, Elizabeth Scotchman, Fiona McKay, Vijaya Ramachandran, Lyn S Chitty
{"title":"Parental Somatic Mosaicism Detected During Prenatal Diagnosis.","authors":"Natalie J Chandler, Elizabeth Scotchman, Fiona McKay, Vijaya Ramachandran, Lyn S Chitty","doi":"10.1002/pd.6712","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Accurate recurrence risks are essential for genomic counselling and parental reproductive choices. Historically, Sanger sequencing was used to test parental samples, which has a limited sensitivity of ∼ 10% for detecting somatic mosaicism. Next generation sequencing (NGS) methods, utilised for non-invasive prenatal diagnosis (NIPD) and trio prenatal exome sequencing in our laboratory, have greater sensitivity. Here we review the cases of parental somatic mosaicism we have detected and discuss its impact on management.</p><p><strong>Method: </strong>Laboratory databases from 1 January 2015 to 30 September 2022 were reviewed to identify all cases where parental somatic mosaicism was detected during NIPD and prenatal exome testing.</p><p><strong>Results: </strong>During the development of NIPD testing, we identified 10/131 (7.6%) families with parental somatic mosaicism. In six cases where NGS detected levels between 0.37% and 8.82%, prior testing with Sanger sequencing had not detected mosaicism. In our exome sequencing cohort, we detected parental mosaicism in 4/101 (3.96%) cases. Clinical features of the condition were identified in 2/14 parents.</p><p><strong>Conclusion: </strong>The sensitivity of the testing technique needs to be considered when counselling parents on recurrence risk. Parents need to be aware that modern approaches to prenatal diagnosis may allow identification of mosaicism, which may have implications for their own health and change recurrence risks for future pregnancies.</p>","PeriodicalId":20387,"journal":{"name":"Prenatal Diagnosis","volume":" ","pages":"171-177"},"PeriodicalIF":2.7000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11790521/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prenatal Diagnosis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pd.6712","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Accurate recurrence risks are essential for genomic counselling and parental reproductive choices. Historically, Sanger sequencing was used to test parental samples, which has a limited sensitivity of ∼ 10% for detecting somatic mosaicism. Next generation sequencing (NGS) methods, utilised for non-invasive prenatal diagnosis (NIPD) and trio prenatal exome sequencing in our laboratory, have greater sensitivity. Here we review the cases of parental somatic mosaicism we have detected and discuss its impact on management.
Method: Laboratory databases from 1 January 2015 to 30 September 2022 were reviewed to identify all cases where parental somatic mosaicism was detected during NIPD and prenatal exome testing.
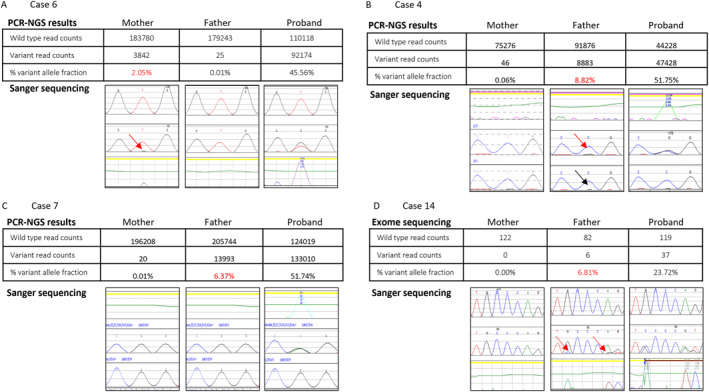
Results: During the development of NIPD testing, we identified 10/131 (7.6%) families with parental somatic mosaicism. In six cases where NGS detected levels between 0.37% and 8.82%, prior testing with Sanger sequencing had not detected mosaicism. In our exome sequencing cohort, we detected parental mosaicism in 4/101 (3.96%) cases. Clinical features of the condition were identified in 2/14 parents.
Conclusion: The sensitivity of the testing technique needs to be considered when counselling parents on recurrence risk. Parents need to be aware that modern approaches to prenatal diagnosis may allow identification of mosaicism, which may have implications for their own health and change recurrence risks for future pregnancies.
期刊介绍:
Prenatal Diagnosis welcomes submissions in all aspects of prenatal diagnosis with a particular focus on areas in which molecular biology and genetics interface with prenatal care and therapy, encompassing: all aspects of fetal imaging, including sonography and magnetic resonance imaging; prenatal cytogenetics, including molecular studies and array CGH; prenatal screening studies; fetal cells and cell-free nucleic acids in maternal blood and other fluids; preimplantation genetic diagnosis (PGD); prenatal diagnosis of single gene disorders, including metabolic disorders; fetal therapy; fetal and placental development and pathology; development and evaluation of laboratory services for prenatal diagnosis; psychosocial, legal, ethical and economic aspects of prenatal diagnosis; prenatal genetic counseling

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


