Matthew Patterson, Pouneh Dokouhaki, Chance S Dumaine, Rebecca MacKay, Davina J Tai
{"title":"Brentuximab-Induced Acute Interstitial Nephritis: A Case Report.","authors":"Matthew Patterson, Pouneh Dokouhaki, Chance S Dumaine, Rebecca MacKay, Davina J Tai","doi":"10.1177/20543581241300766","DOIUrl":null,"url":null,"abstract":"<p><p>Brentuximab vedotin is a combination monoclonal antibody to anti-CD30 conjugated to the anti-tubulin agent monomethyl auristatin E. It is approved for the treatment of mycosis fungoides, Hodgkin's lymphoma, and systemic anaplastic large cell lymphoma. Brentuximab has been associated with a number of potential adverse reactions; however, reports of renal complications are rare. A 73-year-old male with mycosis fungoides was admitted to hospital with acute kidney injury following his third cycle of brentuximab. The patient's serum creatinine (SCr) was 122 µmol/L with an estimated glomerular filtration rate (eGFR) of 58 mL/min/1.73 m<sup>2</sup> at baseline. Following brentuximab, his SCr peaked at 1073 µmol/L over a 4-week period. Acute interstitial nephritis (AIN) was diagnosed after other causes of acute kidney injury were ruled out and subsequently confirmed on kidney biopsy. The patient was started on prednisone 50 mg daily. This was continued for 3 weeks, followed by a 5-week taper. The patient's SCr decreased to 156 µmol/L by completion of the prednisone taper. He was not rechallenged with brentuximab. A kidney biopsy confirmed AIN in keeping with injury from an immune checkpoint inhibitor (ICI). However, brentuximab is not an ICI. The AIN from ICIs typically has tubulointerstitial inflammatory infiltrate comprised of T lymphocytes such as the case presented here. Therefore, this represents both a novel histopathologic finding in AIN from a non-ICI medication and a rare complication of brentuximab, previously only presented in abstract form.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241300766"},"PeriodicalIF":1.5000,"publicationDate":"2024-11-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587173/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241300766","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
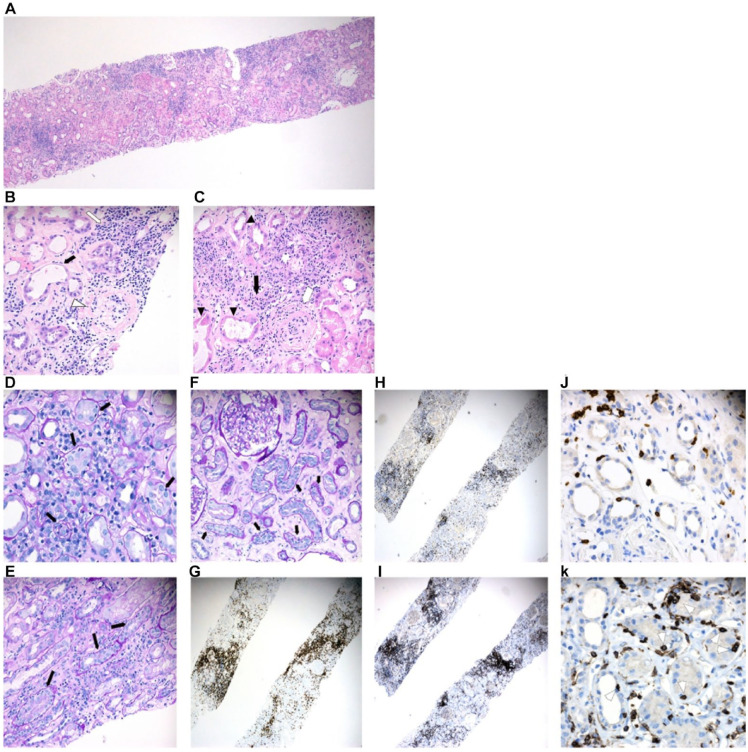
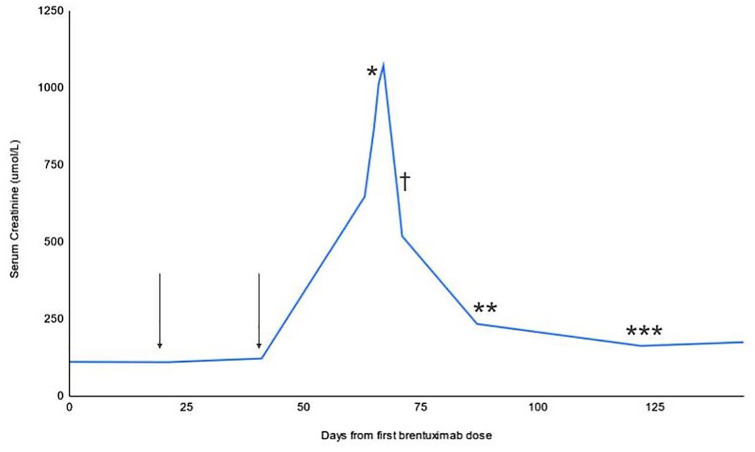
Brentuximab vedotin is a combination monoclonal antibody to anti-CD30 conjugated to the anti-tubulin agent monomethyl auristatin E. It is approved for the treatment of mycosis fungoides, Hodgkin's lymphoma, and systemic anaplastic large cell lymphoma. Brentuximab has been associated with a number of potential adverse reactions; however, reports of renal complications are rare. A 73-year-old male with mycosis fungoides was admitted to hospital with acute kidney injury following his third cycle of brentuximab. The patient's serum creatinine (SCr) was 122 µmol/L with an estimated glomerular filtration rate (eGFR) of 58 mL/min/1.73 m2 at baseline. Following brentuximab, his SCr peaked at 1073 µmol/L over a 4-week period. Acute interstitial nephritis (AIN) was diagnosed after other causes of acute kidney injury were ruled out and subsequently confirmed on kidney biopsy. The patient was started on prednisone 50 mg daily. This was continued for 3 weeks, followed by a 5-week taper. The patient's SCr decreased to 156 µmol/L by completion of the prednisone taper. He was not rechallenged with brentuximab. A kidney biopsy confirmed AIN in keeping with injury from an immune checkpoint inhibitor (ICI). However, brentuximab is not an ICI. The AIN from ICIs typically has tubulointerstitial inflammatory infiltrate comprised of T lymphocytes such as the case presented here. Therefore, this represents both a novel histopathologic finding in AIN from a non-ICI medication and a rare complication of brentuximab, previously only presented in abstract form.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


