Keller and Interphalangeal Joint Resection Arthroplasties for Chronic Noncomplicated Diabetic Ulcers of the Hallux: A Systematic Review and Meta-analysis.
Kaissar Yammine, Joseph Mouawad, Mohammad Omar Honeine, Chahine Assi
{"title":"Keller and Interphalangeal Joint Resection Arthroplasties for Chronic Noncomplicated Diabetic Ulcers of the Hallux: A Systematic Review and Meta-analysis.","authors":"Kaissar Yammine, Joseph Mouawad, Mohammad Omar Honeine, Chahine Assi","doi":"10.1177/24730114241300139","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgery is often needed for resistant plantar diabetic foot ulcers (DFUs) of the big toe. For noninfected ulcers, 2 types of surgery are available: the Keller and the hallux interphalangeal joint arthroplasty (HIPJ-A) procedures. Yet, no evidence synthesis on the outcomes of these procedures has been conducted; thus, this systematic review is an attempt to fill this gap.</p><p><strong>Methods: </strong>Only studies reporting the results of Keller (or its variants) and HIPJ-A (or its variants) procedures for noncomplicated ulcers (Texas 1A/2A, or Wagner I/II) were included. Ulcers located beneath the metatarsal head were excluded. Ultimately, 11 studies were selected for inclusion and were analyzed. The primary outcome was defined as the ulcer healing frequency. The secondary outcomes were mean healing time, ulcer recurrence frequency, ulcer transfer frequency, postoperative infection rate, and revision surgery rate.</p><p><strong>Results: </strong>The overall (combined techniques) weighted healing rate was 94% with a mean healing time of 3.1 ± 0.4 weeks. The ulcer recurrence frequency was 6%, the ulcer transfer frequency 4.5%, the postoperative infection rate 18%, and the revision surgery rate 3.8%. No significant differences were found between both techniques. When compared to standard of care, the odds ratio of ulcer healing frequency was 27.1 (95% CI 1.442-508.174, <i>P</i> = .01) in favor of the Keller arthroplasty with a faster healing time (<i>P</i> = .02).</p><p><strong>Conclusion: </strong>Both surgical offloading procedures are highly effective in treating chronic noncomplicated DFU of the plantar aspect of the hallux along with low complication frequencies. There is a need to fine-tune the indication in relation to the location of the plantar wound with future comparative controlled research studies with far more patients than we could include in this meta-analysis.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"9 4","pages":"24730114241300139"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11585028/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114241300139","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Surgery is often needed for resistant plantar diabetic foot ulcers (DFUs) of the big toe. For noninfected ulcers, 2 types of surgery are available: the Keller and the hallux interphalangeal joint arthroplasty (HIPJ-A) procedures. Yet, no evidence synthesis on the outcomes of these procedures has been conducted; thus, this systematic review is an attempt to fill this gap.
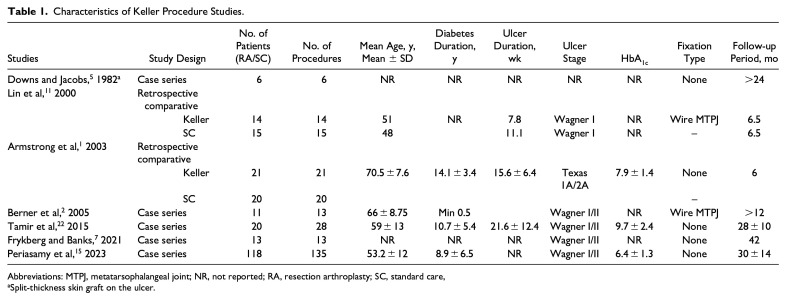
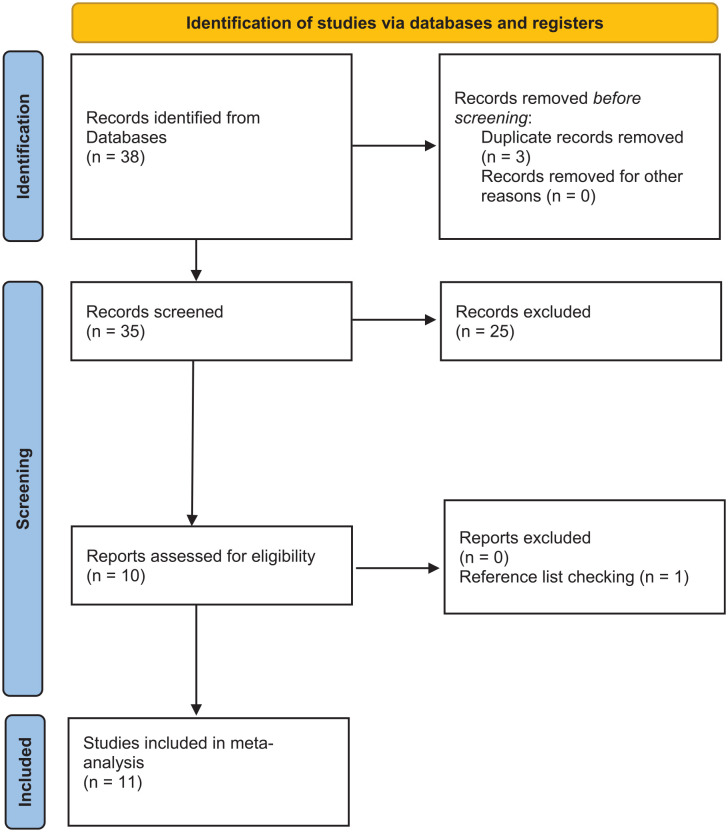
Methods: Only studies reporting the results of Keller (or its variants) and HIPJ-A (or its variants) procedures for noncomplicated ulcers (Texas 1A/2A, or Wagner I/II) were included. Ulcers located beneath the metatarsal head were excluded. Ultimately, 11 studies were selected for inclusion and were analyzed. The primary outcome was defined as the ulcer healing frequency. The secondary outcomes were mean healing time, ulcer recurrence frequency, ulcer transfer frequency, postoperative infection rate, and revision surgery rate.
Results: The overall (combined techniques) weighted healing rate was 94% with a mean healing time of 3.1 ± 0.4 weeks. The ulcer recurrence frequency was 6%, the ulcer transfer frequency 4.5%, the postoperative infection rate 18%, and the revision surgery rate 3.8%. No significant differences were found between both techniques. When compared to standard of care, the odds ratio of ulcer healing frequency was 27.1 (95% CI 1.442-508.174, P = .01) in favor of the Keller arthroplasty with a faster healing time (P = .02).
Conclusion: Both surgical offloading procedures are highly effective in treating chronic noncomplicated DFU of the plantar aspect of the hallux along with low complication frequencies. There is a need to fine-tune the indication in relation to the location of the plantar wound with future comparative controlled research studies with far more patients than we could include in this meta-analysis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


