{"title":"Ecthyma Gangrenosum of Fungal Origin: A Case Report.","authors":"Germán Andrés León-Sánchez, Heiler Lozada-Ramos, Jorge Enrique Daza-Arana, Andrés Darío Restrepo-Becerra, Ruben Varela-Miranda","doi":"10.1159/000542105","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Ecthyma gangrenosum (EG) is usually a dermatologic manifestation of a <i>Pseudomonas aeruginosa</i> infection in an immunocompromised individual but may sometimes be caused by other bacteria or fungi in an immunocompromised or non-immunocompromised individual.</p><p><strong>Case presentation: </strong>A 75-year-old woman with a history of high blood pressure and sequels of ischemic cerebral infarction presented with a 5-day history of general malaise, cough with yellow sputum, and respiratory distress. The patient had pale mucous membranes, temperature of 38.5°C, tachycardia, normal blood pressure, SaO<sub>2</sub> of 85%, intercostal retractions, and severe bronchospasm upon hospital admission. No skin lesions were seen. The patient was admitted to the intensive care unit (ICU) because of her critical condition and was supported with invasive mechanical ventilation. Her blood count showed 8,100 leukocytes/mm<sup>3</sup>, neutrophils 79%, hemoglobin 10.1 g/dL, creatinine 1.1 mg/dL, and C-reactive protein 328 mg/dL. Arterial blood gases showed metabolic acidosis and moderate hypoxemia. The initial report of blood and urine cultures was negative for bacteria, and positive for influenza A H1N1. The patient was treated with oseltamivir and intravenous methylprednisolone for acute respiratory distress syndrome associated with the viral infection that occurred. Subsequently, violaceus macular and papular lesions appeared, which evolved into ulcerated lesions with erythematous border and necrotic center were seen in the anterior region of the chest and abdomen, from where <i>Candida metapsilosis</i> was isolated. EG was reported in this patient, who was also immunocompromised because of steroid use, had a prolonged stay in the ICU and received broad-spectrum antibiotics. Fungemia and urinary infection due to different fungi were also found.</p><p><strong>Conclusion: </strong>It is worth mentioning that EG can be caused by germs other than <i>P. aeruginosa</i> and fungal infections should not be ruled out.</p>","PeriodicalId":9619,"journal":{"name":"Case Reports in Dermatology","volume":"16 1","pages":"240-247"},"PeriodicalIF":0.8000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584198/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Dermatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000542105","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Ecthyma gangrenosum (EG) is usually a dermatologic manifestation of a Pseudomonas aeruginosa infection in an immunocompromised individual but may sometimes be caused by other bacteria or fungi in an immunocompromised or non-immunocompromised individual.
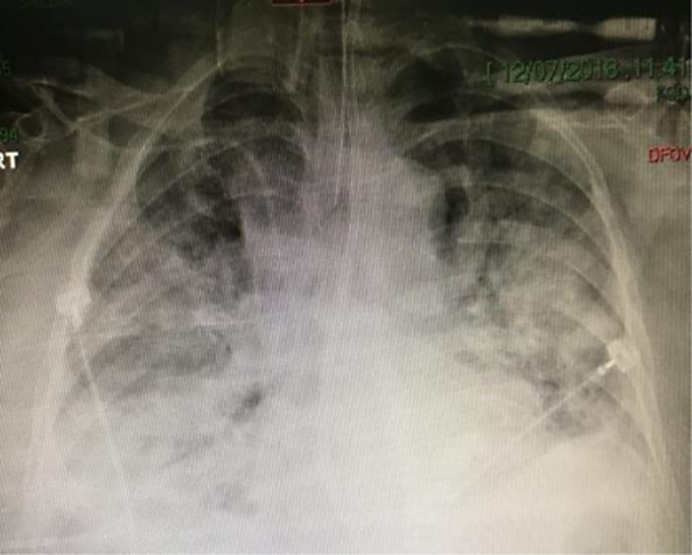
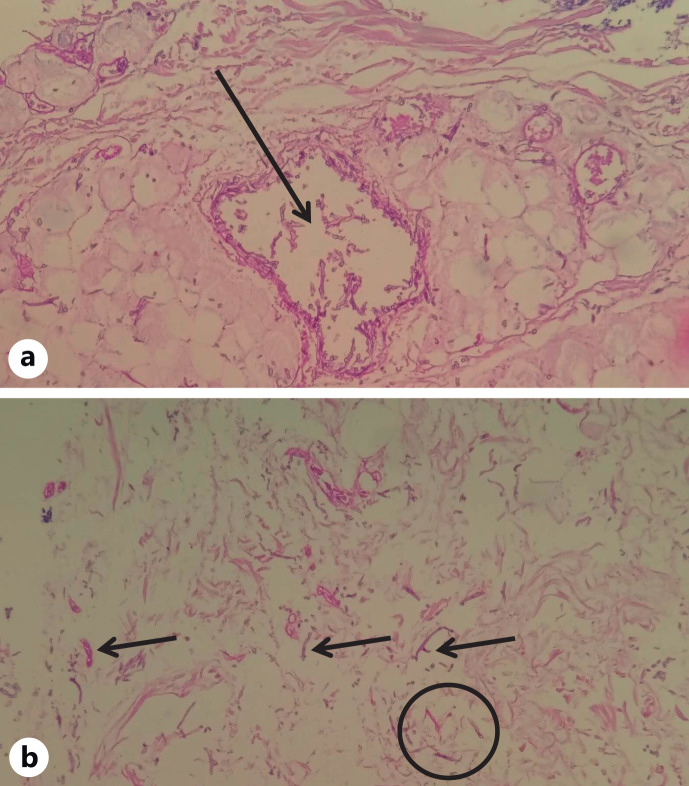
Case presentation: A 75-year-old woman with a history of high blood pressure and sequels of ischemic cerebral infarction presented with a 5-day history of general malaise, cough with yellow sputum, and respiratory distress. The patient had pale mucous membranes, temperature of 38.5°C, tachycardia, normal blood pressure, SaO2 of 85%, intercostal retractions, and severe bronchospasm upon hospital admission. No skin lesions were seen. The patient was admitted to the intensive care unit (ICU) because of her critical condition and was supported with invasive mechanical ventilation. Her blood count showed 8,100 leukocytes/mm3, neutrophils 79%, hemoglobin 10.1 g/dL, creatinine 1.1 mg/dL, and C-reactive protein 328 mg/dL. Arterial blood gases showed metabolic acidosis and moderate hypoxemia. The initial report of blood and urine cultures was negative for bacteria, and positive for influenza A H1N1. The patient was treated with oseltamivir and intravenous methylprednisolone for acute respiratory distress syndrome associated with the viral infection that occurred. Subsequently, violaceus macular and papular lesions appeared, which evolved into ulcerated lesions with erythematous border and necrotic center were seen in the anterior region of the chest and abdomen, from where Candida metapsilosis was isolated. EG was reported in this patient, who was also immunocompromised because of steroid use, had a prolonged stay in the ICU and received broad-spectrum antibiotics. Fungemia and urinary infection due to different fungi were also found.
Conclusion: It is worth mentioning that EG can be caused by germs other than P. aeruginosa and fungal infections should not be ruled out.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


