Adjuvant chemotherapy for isolated resectable colorectal lung metastasis: A retrospective study using inverse probability treatment weighting propensity analysis.
Zhao Gao, Shi-Kai Wu, Shi-Jie Zhang, Xin Wang, Ying-Chao Wu, Xuan Jin
{"title":"Adjuvant chemotherapy for isolated resectable colorectal lung metastasis: A retrospective study using inverse probability treatment weighting propensity analysis.","authors":"Zhao Gao, Shi-Kai Wu, Shi-Jie Zhang, Xin Wang, Ying-Chao Wu, Xuan Jin","doi":"10.4240/wjgs.v16.i10.3171","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The benefit of adjuvant chemotherapy (ACT) for patients with no evidence of disease after pulmonary metastasis resection (PM) from colorectal cancer (CRC) remains controversial.</p><p><strong>Aim: </strong>To assess the efficacy of ACT in patients after PM resection for CRC.</p><p><strong>Methods: </strong>This study included 96 patients who underwent pulmonary metastasectomy for CRC at a single institution between April 2008 and July 2023. The primary endpoint was overall survival (OS); secondary endpoints included cancer-specific survival (CSS) and disease-free survival (DFS). An inverse probability of treatment-weighting (IPTW) analysis was conducted to address indication bias. Survival outcomes compared using Kaplan-Meier curves, log-rank test, Cox regression and confirmed by propensity score-matching (PSM).</p><p><strong>Results: </strong>With a median follow-up of 27.5 months (range, 18.3-50.4 months), the 5-year OS, CSS and DFS were 72.0%, 74.4% and 51.3%, respectively. ACT had no significant effect on OS after PM resection from CRC [original cohort: <i>P</i> = 0.08; IPTW: <i>P</i> = 0.15]. No differences were observed for CSS (<i>P</i> = 0.12) and DFS (<i>P</i> = 0.68) between the ACT and non-ACT groups. Multivariate analysis showed no association of ACT with better survival, while sublobar resection (HR = 0.45; 95%CI: 0.20-1.00, <i>P</i> = 0.049) and longer disease-free interval (HR = 0.45; 95%CI: 0.20-0.98, <i>P</i> = 0.044) were associated with improved survival.</p><p><strong>Conclusion: </strong>ACT does not improve survival after PM resection for CRC. Further well-designed randomized controlled trials are needed to determine the optimal ACT regimen and duration.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"16 10","pages":"3171-3184"},"PeriodicalIF":1.7000,"publicationDate":"2024-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11577391/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v16.i10.3171","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The benefit of adjuvant chemotherapy (ACT) for patients with no evidence of disease after pulmonary metastasis resection (PM) from colorectal cancer (CRC) remains controversial.
Aim: To assess the efficacy of ACT in patients after PM resection for CRC.
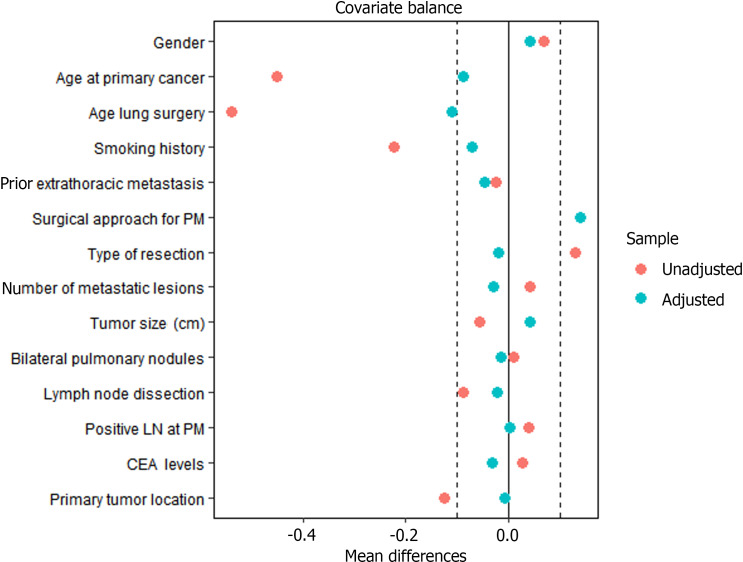
Methods: This study included 96 patients who underwent pulmonary metastasectomy for CRC at a single institution between April 2008 and July 2023. The primary endpoint was overall survival (OS); secondary endpoints included cancer-specific survival (CSS) and disease-free survival (DFS). An inverse probability of treatment-weighting (IPTW) analysis was conducted to address indication bias. Survival outcomes compared using Kaplan-Meier curves, log-rank test, Cox regression and confirmed by propensity score-matching (PSM).
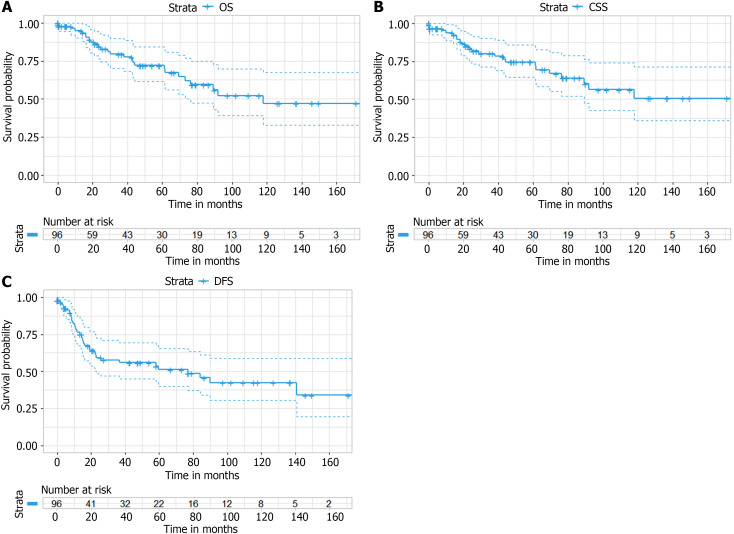
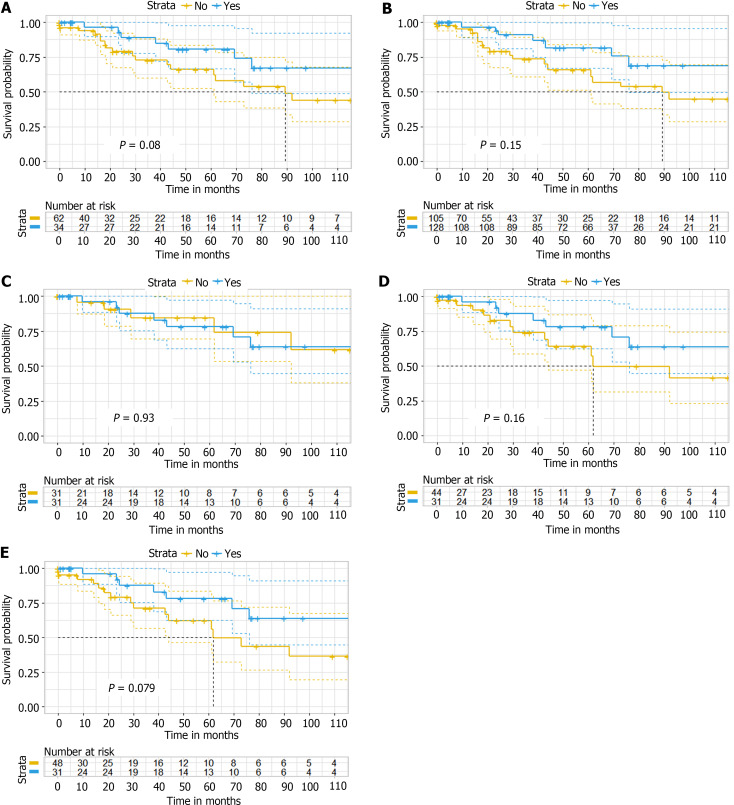
Results: With a median follow-up of 27.5 months (range, 18.3-50.4 months), the 5-year OS, CSS and DFS were 72.0%, 74.4% and 51.3%, respectively. ACT had no significant effect on OS after PM resection from CRC [original cohort: P = 0.08; IPTW: P = 0.15]. No differences were observed for CSS (P = 0.12) and DFS (P = 0.68) between the ACT and non-ACT groups. Multivariate analysis showed no association of ACT with better survival, while sublobar resection (HR = 0.45; 95%CI: 0.20-1.00, P = 0.049) and longer disease-free interval (HR = 0.45; 95%CI: 0.20-0.98, P = 0.044) were associated with improved survival.
Conclusion: ACT does not improve survival after PM resection for CRC. Further well-designed randomized controlled trials are needed to determine the optimal ACT regimen and duration.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


