Samuel Heuts, Michal J Kawczynski, Arthur Leus, Laurent Godinas, Catharina Belge, Vanessa van Empel, Bart Meyns, Jos G Maessen, Marion Delcroix, Tom Verbelen
{"title":"The volume-outcome relationship for pulmonary endarterectomy in chronic thromboembolic pulmonary hypertension.","authors":"Samuel Heuts, Michal J Kawczynski, Arthur Leus, Laurent Godinas, Catharina Belge, Vanessa van Empel, Bart Meyns, Jos G Maessen, Marion Delcroix, Tom Verbelen","doi":"10.1183/13993003.01865-2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We conducted a volume-outcome meta-analysis of pulmonary endarterectomy procedures for chronic thromboembolic pulmonary hypertension to objectively determine the minimum required annual case load that can define a high-volume centre.</p><p><strong>Methods: </strong>Three electronic databases were systematically queried up to 1 May 2024. Centres were divided in volume tertiles. The primary outcomes were early mortality and long-term survival. Restricted cubic splines were used to demonstrate the volume-outcome relationship and the elbow-method was applied to define high-volume centres. Long-term survival was assessed using Cox frailty models.</p><p><strong>Results: </strong>We included 51 centres (52 consecutive cohorts) and divided them into tertiles (T1: <6 cases per year; T2: 6-15 cases per year, T3: >15 cases per year), comprising a total 11 345 patients (mean age 52.3 years). Overall early mortality was 6.0% (T1: 11.6%; T2: 7.2%; T3: 5.2%; p<0.001), for which a significant nonlinear volume-outcome relationship was observed (p=0.0437) with a statistically determined minimal required volume of 33 cases per year (95% CI 29-35 cases), and a modelled volume of 40 cases per year corresponding to a 5.0% mortality rate. Nevertheless, early mortality still progressively declined in higher volume centres (from 6.7% to 5.4% to 2.9% in centres performing 16-50, 51-100 and >100 procedures annually). In addition, a significant volume effect was observed for long-term survival (adjusted hazard ratio per tertile 0.75, 95% CI 0.63-0.89; p=0.001).</p><p><strong>Conclusion: </strong>There is a significant association between procedural volume and early mortality in pulmonary endarterectomy. An annual procedural volume of >33-40 cases per year may be used to define a high‑volume centre, although higher volumes still lead to progressively lower mortality rates.</p>","PeriodicalId":12265,"journal":{"name":"European Respiratory Journal","volume":" ","pages":""},"PeriodicalIF":21.0000,"publicationDate":"2025-02-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11865742/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Respiratory Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1183/13993003.01865-2024","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"Print","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We conducted a volume-outcome meta-analysis of pulmonary endarterectomy procedures for chronic thromboembolic pulmonary hypertension to objectively determine the minimum required annual case load that can define a high-volume centre.
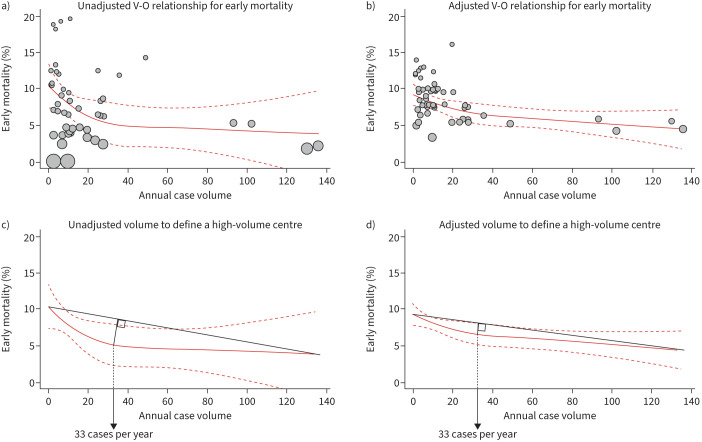
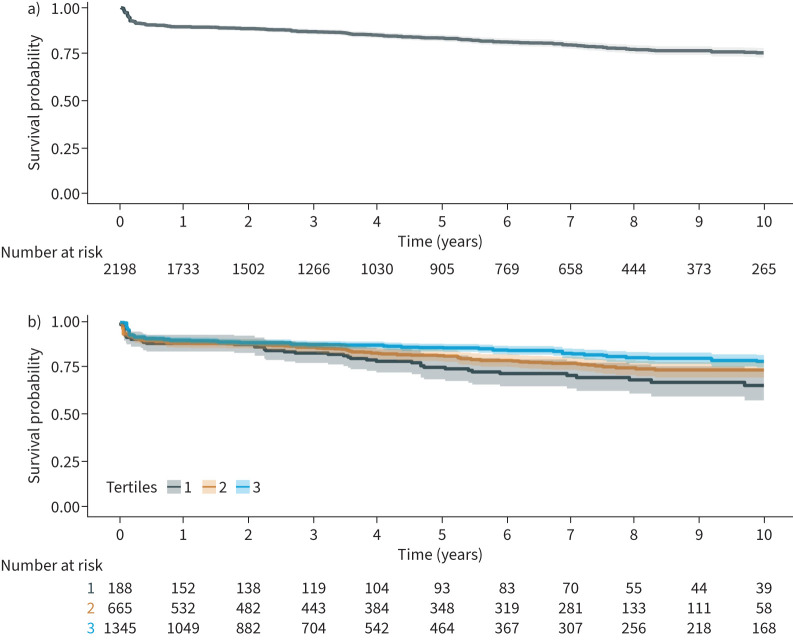
Methods: Three electronic databases were systematically queried up to 1 May 2024. Centres were divided in volume tertiles. The primary outcomes were early mortality and long-term survival. Restricted cubic splines were used to demonstrate the volume-outcome relationship and the elbow-method was applied to define high-volume centres. Long-term survival was assessed using Cox frailty models.
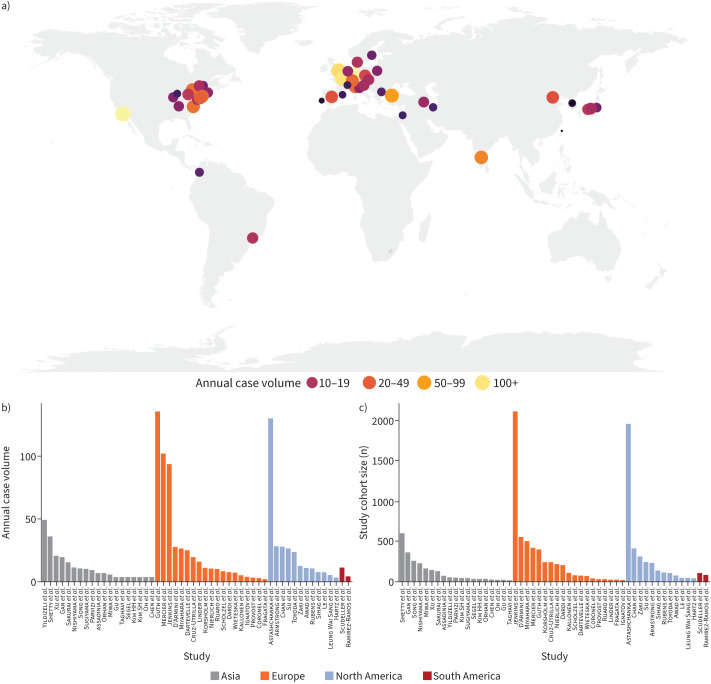
Results: We included 51 centres (52 consecutive cohorts) and divided them into tertiles (T1: <6 cases per year; T2: 6-15 cases per year, T3: >15 cases per year), comprising a total 11 345 patients (mean age 52.3 years). Overall early mortality was 6.0% (T1: 11.6%; T2: 7.2%; T3: 5.2%; p<0.001), for which a significant nonlinear volume-outcome relationship was observed (p=0.0437) with a statistically determined minimal required volume of 33 cases per year (95% CI 29-35 cases), and a modelled volume of 40 cases per year corresponding to a 5.0% mortality rate. Nevertheless, early mortality still progressively declined in higher volume centres (from 6.7% to 5.4% to 2.9% in centres performing 16-50, 51-100 and >100 procedures annually). In addition, a significant volume effect was observed for long-term survival (adjusted hazard ratio per tertile 0.75, 95% CI 0.63-0.89; p=0.001).
Conclusion: There is a significant association between procedural volume and early mortality in pulmonary endarterectomy. An annual procedural volume of >33-40 cases per year may be used to define a high‑volume centre, although higher volumes still lead to progressively lower mortality rates.
期刊介绍:
The European Respiratory Journal (ERJ) is the flagship journal of the European Respiratory Society. It has a current impact factor of 24.9. The journal covers various aspects of adult and paediatric respiratory medicine, including cell biology, epidemiology, immunology, oncology, pathophysiology, imaging, occupational medicine, intensive care, sleep medicine, and thoracic surgery. In addition to original research material, the ERJ publishes editorial commentaries, reviews, short research letters, and correspondence to the editor. The articles are published continuously and collected into 12 monthly issues in two volumes per year.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


