Diuretic treatment using the RenalGuard® system in patients hospitalized due to acute decompensated heart failure and characterization of the profile of patients with good and poor response to treatment - preliminary study.
Paweł Siwołowski, Piotr Gajewski, Mateusz Sokolski, Robert Zymliński, Mateusz Guzik, Joanna Szachniewicz, Piotr Ponikowski
{"title":"Diuretic treatment using the RenalGuard® system in patients hospitalized due to acute decompensated heart failure and characterization of the profile of patients with good and poor response to treatment - preliminary study.","authors":"Paweł Siwołowski, Piotr Gajewski, Mateusz Sokolski, Robert Zymliński, Mateusz Guzik, Joanna Szachniewicz, Piotr Ponikowski","doi":"10.5603/cj.102386","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of the study was to analyze the potential relationship between the diuretic response, the clinical profile and the concentrations of selected biochemical markers and to identify a group of patients who will benefit from a new form of therapy combining standard diuretic therapy with the use of a RenalGuard® system.</p><p><strong>Methods: </strong>This is a retrospective study of 19 patients (mean age 67 ± 10 years, 95% men) hospitalized due to acute decompensated heart failure (ADHF, NYHA class III-IV, BP 125 ± 14/73 ± 16 mmHg, eGFR 58 ± 24) with persistent overhydration despite standard therapy. A targeted comparative analysis of selected clinical and biochemical parameters was performed to determine the parameters associated with a better diuretic response [good diuretic responders (GDR) group].</p><p><strong>Results: </strong>The good diuretic responders group had significantly lower levels of creatinine (1.23 ± 0.4 vs. 1.69 ± 0.35, p = 0.025) magnesium 0.70 ± 0.14 vs. 0.83 ± 0.09, p = 0.030) and blood urea nitrogen (BUN, 28 ± 11 vs. 39 ± 10, p = 0.045). Additionally, in GDR group a statistically significant greater ability to dilute urine in the 12th and 24th hour of therapy was found.</p><p><strong>Conclusions: </strong>The results of the study indicate the potential use of the RenalGuard® system in combination with standard intravenous diuretic therapy for controlled dehydration in the treatment of a selected group of patients with ADHF. It is advisable to identify the detailed mechanisms of GDR and characterize this group of patients more precisely.</p>","PeriodicalId":93923,"journal":{"name":"Cardiology journal","volume":" ","pages":"43-52"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11870006/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5603/cj.102386","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The aim of the study was to analyze the potential relationship between the diuretic response, the clinical profile and the concentrations of selected biochemical markers and to identify a group of patients who will benefit from a new form of therapy combining standard diuretic therapy with the use of a RenalGuard® system.
Methods: This is a retrospective study of 19 patients (mean age 67 ± 10 years, 95% men) hospitalized due to acute decompensated heart failure (ADHF, NYHA class III-IV, BP 125 ± 14/73 ± 16 mmHg, eGFR 58 ± 24) with persistent overhydration despite standard therapy. A targeted comparative analysis of selected clinical and biochemical parameters was performed to determine the parameters associated with a better diuretic response [good diuretic responders (GDR) group].
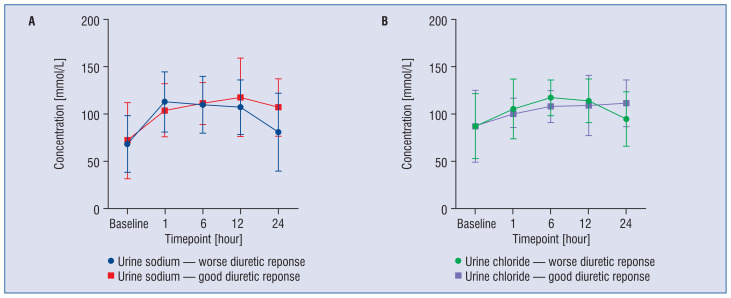
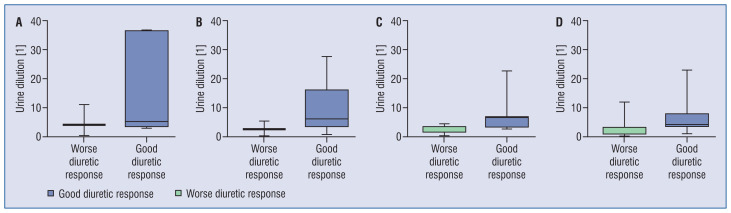
Results: The good diuretic responders group had significantly lower levels of creatinine (1.23 ± 0.4 vs. 1.69 ± 0.35, p = 0.025) magnesium 0.70 ± 0.14 vs. 0.83 ± 0.09, p = 0.030) and blood urea nitrogen (BUN, 28 ± 11 vs. 39 ± 10, p = 0.045). Additionally, in GDR group a statistically significant greater ability to dilute urine in the 12th and 24th hour of therapy was found.
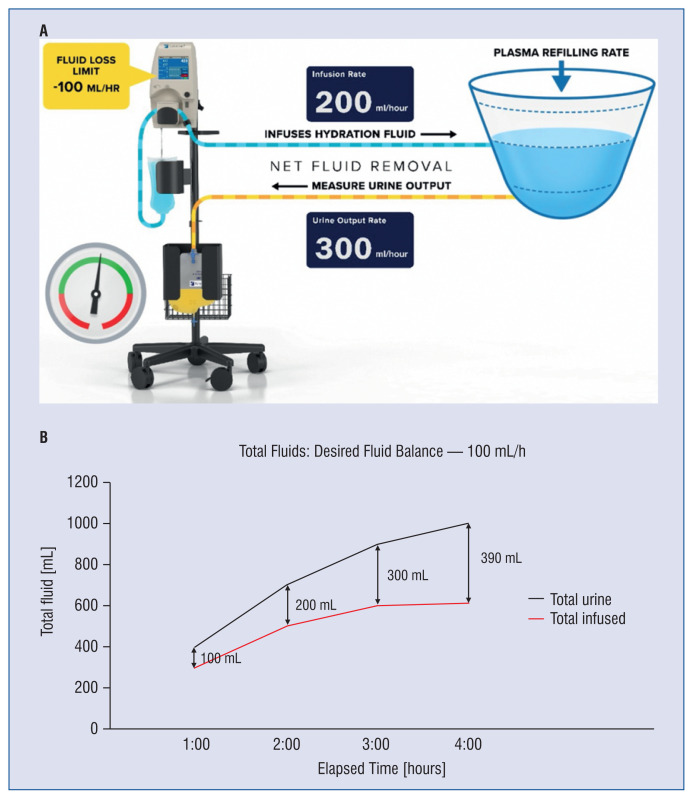
Conclusions: The results of the study indicate the potential use of the RenalGuard® system in combination with standard intravenous diuretic therapy for controlled dehydration in the treatment of a selected group of patients with ADHF. It is advisable to identify the detailed mechanisms of GDR and characterize this group of patients more precisely.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


