Basilia Anabel Cahuich-Rodríguez, Arlene Guadalupe Acosta-Mass, Héctor Isaac Rocha-González
{"title":"[Risk of postoperative delirium in older adults under balanced general anesthesia].","authors":"Basilia Anabel Cahuich-Rodríguez, Arlene Guadalupe Acosta-Mass, Héctor Isaac Rocha-González","doi":"10.5281/zenodo.13381460","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anesthetic depth can influence the incidence of postoperative delirium (POD). This depth is related to the potency of the volatile anesthetics used to maintain balanced general anesthesia. This potency is measured by means of the minimum alveolar concentration (MAC). In older adults, it is unknown which MAC is associated with the risk of POD.</p><p><strong>Objective: </strong>To estimate the risk of POD associated with minimum alveolar concentration (MAC) levels of volatile anesthetics in older adults who received balanced general anesthesia.</p><p><strong>Material and methods: </strong>A prospective cohort study was carried out with 119 patients, aged ≥ 60 years, with 0 points in the 4 \"As\" test (4AT), without neurological or psychiatric diseases. During the intraoperative period, the CAM provided was recorded, and in the postoperative period, the presence of emergency with delirium and/or POD was evaluated at 2 and 24 hours, considering a score ≥ 4.</p><p><strong>Results: </strong>A longer hospital stay was found in the group that received a MAC ≥0.9. The incidence of POD was 29.4%. Those who received a MAC ≥ 0.9 had an RR of 2.22 (95%CI: 1.2-4.2) of presenting POD. An adjusted logistic regression model was performed with the variables female sex (OR: 4, 95%CI: 1.5-10.4), ASA physical status 3-4 (OR: 3.7, 95%CI: 1.5-9) and MAC ≥ 0.9 (OR: 3.1 95%CI: 1.2-8) with an R2: 0.26 and a constant of 3.005.</p><p><strong>Conclusions: </strong>MAC ≥ 0.9 represents a risk factor for DPO, so individualized dosing of volatile anesthetics should be used.</p>","PeriodicalId":94200,"journal":{"name":"Revista medica del Instituto Mexicano del Seguro Social","volume":"62 6","pages":"1-8"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12527409/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista medica del Instituto Mexicano del Seguro Social","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5281/zenodo.13381460","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Anesthetic depth can influence the incidence of postoperative delirium (POD). This depth is related to the potency of the volatile anesthetics used to maintain balanced general anesthesia. This potency is measured by means of the minimum alveolar concentration (MAC). In older adults, it is unknown which MAC is associated with the risk of POD.
Objective: To estimate the risk of POD associated with minimum alveolar concentration (MAC) levels of volatile anesthetics in older adults who received balanced general anesthesia.
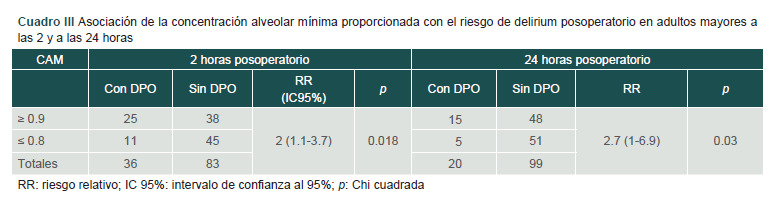
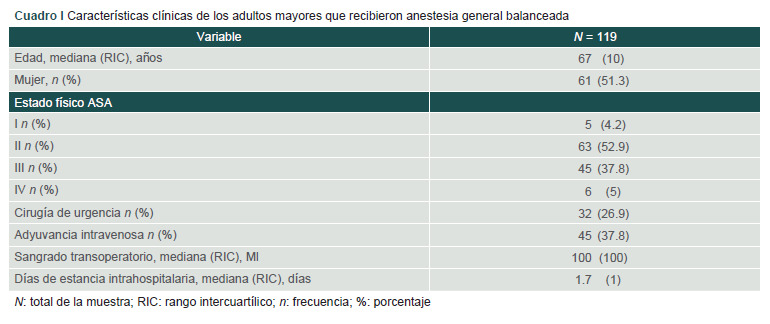
Material and methods: A prospective cohort study was carried out with 119 patients, aged ≥ 60 years, with 0 points in the 4 "As" test (4AT), without neurological or psychiatric diseases. During the intraoperative period, the CAM provided was recorded, and in the postoperative period, the presence of emergency with delirium and/or POD was evaluated at 2 and 24 hours, considering a score ≥ 4.
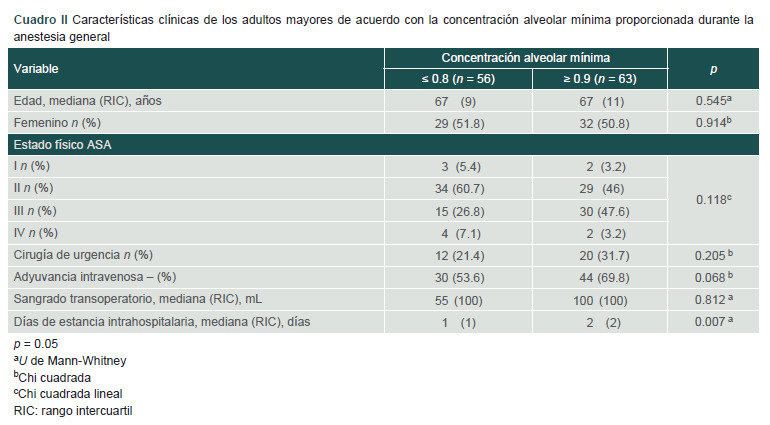
Results: A longer hospital stay was found in the group that received a MAC ≥0.9. The incidence of POD was 29.4%. Those who received a MAC ≥ 0.9 had an RR of 2.22 (95%CI: 1.2-4.2) of presenting POD. An adjusted logistic regression model was performed with the variables female sex (OR: 4, 95%CI: 1.5-10.4), ASA physical status 3-4 (OR: 3.7, 95%CI: 1.5-9) and MAC ≥ 0.9 (OR: 3.1 95%CI: 1.2-8) with an R2: 0.26 and a constant of 3.005.
Conclusions: MAC ≥ 0.9 represents a risk factor for DPO, so individualized dosing of volatile anesthetics should be used.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


