Clinical evolution of gallstones following percutaneous cholecystostomy in patients with severe acute calculous cholecystitis: a single-center analysis of 102 cases.
Ram Ragatha, Ibraheem Khalil, Rebecca Jones, Antonio Manzelli, Alex Reece-Smith, Yunli Ou, Shahjehan Wajed, Davide Di Mauro
{"title":"Clinical evolution of gallstones following percutaneous cholecystostomy in patients with severe acute calculous cholecystitis: a single-center analysis of 102 cases.","authors":"Ram Ragatha, Ibraheem Khalil, Rebecca Jones, Antonio Manzelli, Alex Reece-Smith, Yunli Ou, Shahjehan Wajed, Davide Di Mauro","doi":"10.20524/aog.2024.0915","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Percutaneous cholecystostomy (PC) is effective in controlling sepsis in patients with severe acute calculous cholecystitis (ACC). The long-term treatment of this group is still debated. We aimed to assess the clinical evolution of gallstones after severe ACC and the outcomes of laparoscopic cholecystectomy (LC) and conservative management, following PC.</p><p><strong>Methods: </strong>This was a retrospective analysis of the rate of readmissions due to recurrent biliary disease and all-cause mortality in subjects who underwent a PC for severe ACC. We compared results between patients who underwent interval LC and those who received conservative management. Readmissions and late mortality were assessed using the Kaplan-Meier method and multivariate regression analysis.</p><p><strong>Results: </strong>A total of 102 patients were included, of whom 30 underwent interval LC and 72 PC only. Overall, 51.6% were readmitted with recurrent biliary events and the rate did not differ between groups (P=0.583). The probability of recurrent gallstone events was higher in the first 30 weeks after PC; in the surgical cohort, 77.8% of them developed before LC. Late deaths occurred in 46.2% of patients: 13.3% LC vs. 61.9% conservative (P<0.001). Three years after PC, the estimated survival was 75% LC vs. 38% conservative (P=0.014). High-grade comorbidities and severity of ACC were positive predictors of all-cause mortality (P=0.004 and P=0.027), whereas LC was a negative predictor (P=0.003).</p><p><strong>Conclusions: </strong>Recurrent biliary events were common following PC for ACC. Interval LC was associated with lower rates of readmissions and all-cause late mortality.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 6","pages":"718-725"},"PeriodicalIF":2.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574151/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0915","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Percutaneous cholecystostomy (PC) is effective in controlling sepsis in patients with severe acute calculous cholecystitis (ACC). The long-term treatment of this group is still debated. We aimed to assess the clinical evolution of gallstones after severe ACC and the outcomes of laparoscopic cholecystectomy (LC) and conservative management, following PC.
Methods: This was a retrospective analysis of the rate of readmissions due to recurrent biliary disease and all-cause mortality in subjects who underwent a PC for severe ACC. We compared results between patients who underwent interval LC and those who received conservative management. Readmissions and late mortality were assessed using the Kaplan-Meier method and multivariate regression analysis.
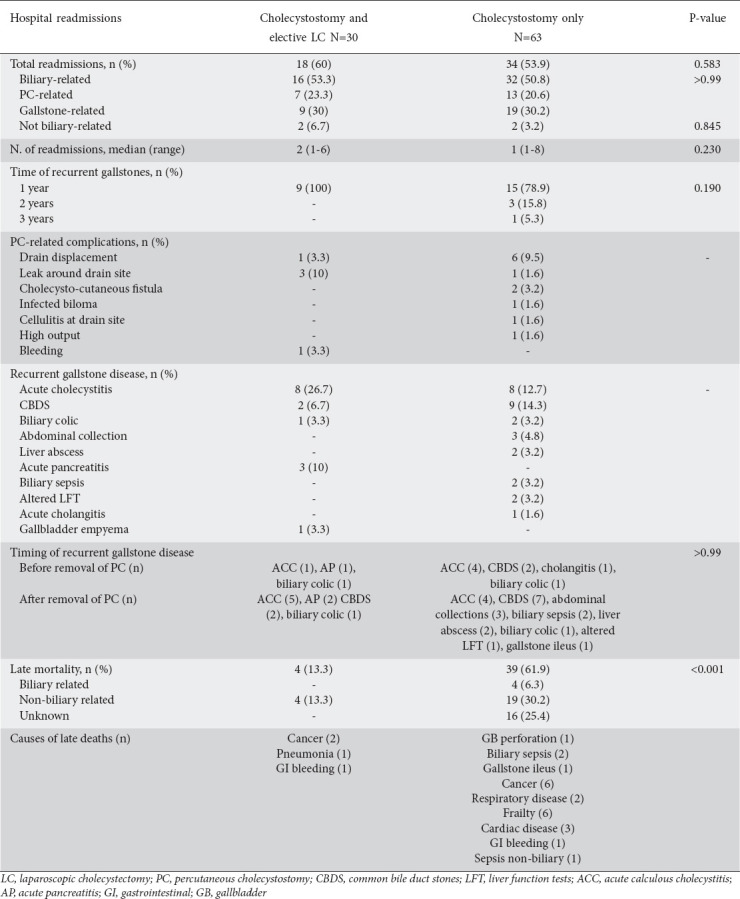
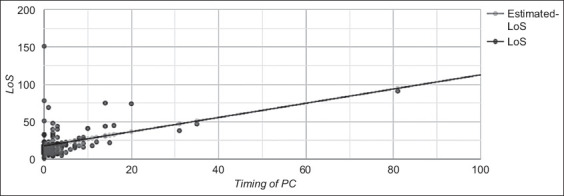
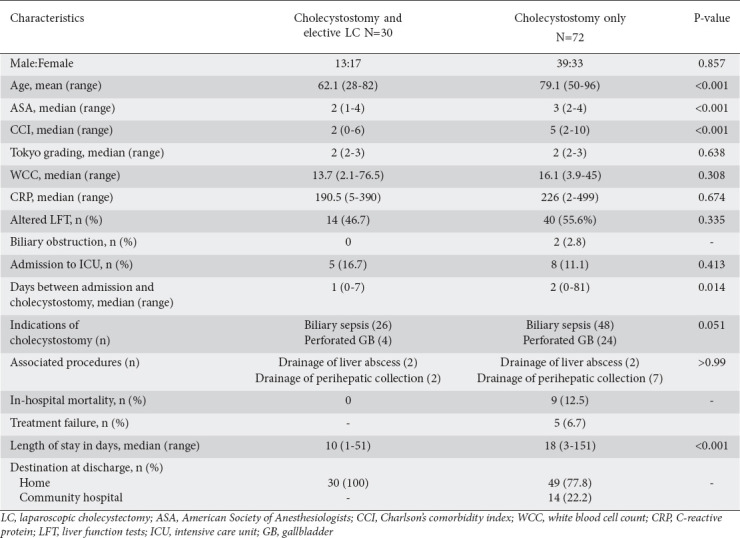
Results: A total of 102 patients were included, of whom 30 underwent interval LC and 72 PC only. Overall, 51.6% were readmitted with recurrent biliary events and the rate did not differ between groups (P=0.583). The probability of recurrent gallstone events was higher in the first 30 weeks after PC; in the surgical cohort, 77.8% of them developed before LC. Late deaths occurred in 46.2% of patients: 13.3% LC vs. 61.9% conservative (P<0.001). Three years after PC, the estimated survival was 75% LC vs. 38% conservative (P=0.014). High-grade comorbidities and severity of ACC were positive predictors of all-cause mortality (P=0.004 and P=0.027), whereas LC was a negative predictor (P=0.003).
Conclusions: Recurrent biliary events were common following PC for ACC. Interval LC was associated with lower rates of readmissions and all-cause late mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


