Real-world outcomes of collaborative surgery for gastrointestinal tumors by endoscopists and surgeons: a single-center retrospective analysis of 131 patients.
{"title":"Real-world outcomes of collaborative surgery for gastrointestinal tumors by endoscopists and surgeons: a single-center retrospective analysis of 131 patients.","authors":"Kazutoshi Higuchi, Osamu Goto, Nobuyuki Sakurazawa, Atsuko Sakanushi, Koji Sakamoto, Akira Matsushita, Nobutoshi Hagiwara, Akihisa Matsuda, Toshihiko Hoashi, Shun Nakagome, Tsugumi Habu, Yumiko Ishikawa, Eriko Koizumi, Jun Omori, Naohiko Akimoto, Ryuji Ohashi, Hidehisa Saeki, Kimihiro Okubo, Hiroshi Yoshida, Katsuhiko Iwakiri","doi":"10.20524/aog.2024.0921","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Collaborative surgery by both endoscopists and surgeons is considered effective for providing less invasive local resection of gastrointestinal tumors, to offset the limitations of either pure endoscopic treatments or surgical intervention. The clinical outcomes of collaborative surgery were evaluated to investigate the feasibility and safety of this approach.</p><p><strong>Methods: </strong>In this single-center retrospective observational study, we collected data from consecutive patients who underwent collaborative surgery for lesions located from the laryngopharynx to the anus. The completeness of collaboration, technical success, procedure time, postoperative hospitalization period, and occurrence of adverse events were analyzed.</p><p><strong>Results: </strong>Collaboration surgery was performed for 134 lesions (33 laryngopharyngeal, 2 esophageal, 89 gastric, 8 duodenal and 2 recto-anal) in 131 patients. Collaboration completeness was achieved in 129 lesions (96%). <i>En bloc</i> resection and pathological R0 resection of lesions were achieved in 127 (95%) and 124 (93%) lesions, respectively. The mean procedure time was 188 min. The mean time of discharge was the 11<sup>th</sup> postoperative day. Five patients (4%) developed relevant postoperative adverse events.</p><p><strong>Conclusions: </strong>These results indicate that collaborative surgery by endoscopists and surgeons was feasible and safe, and may contribute to providing less invasive treatment than conventional surgery. Collaborative surgery is worth considering as a flexible and reliable surgical option, when cooperation may outperform either treatment alone.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 6","pages":"699-707"},"PeriodicalIF":2.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11574152/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0921","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Collaborative surgery by both endoscopists and surgeons is considered effective for providing less invasive local resection of gastrointestinal tumors, to offset the limitations of either pure endoscopic treatments or surgical intervention. The clinical outcomes of collaborative surgery were evaluated to investigate the feasibility and safety of this approach.
Methods: In this single-center retrospective observational study, we collected data from consecutive patients who underwent collaborative surgery for lesions located from the laryngopharynx to the anus. The completeness of collaboration, technical success, procedure time, postoperative hospitalization period, and occurrence of adverse events were analyzed.
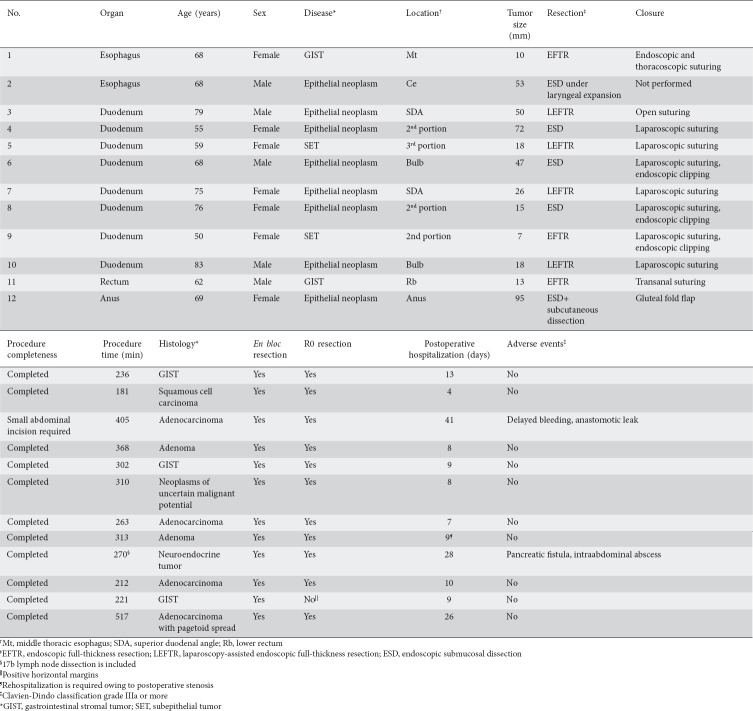
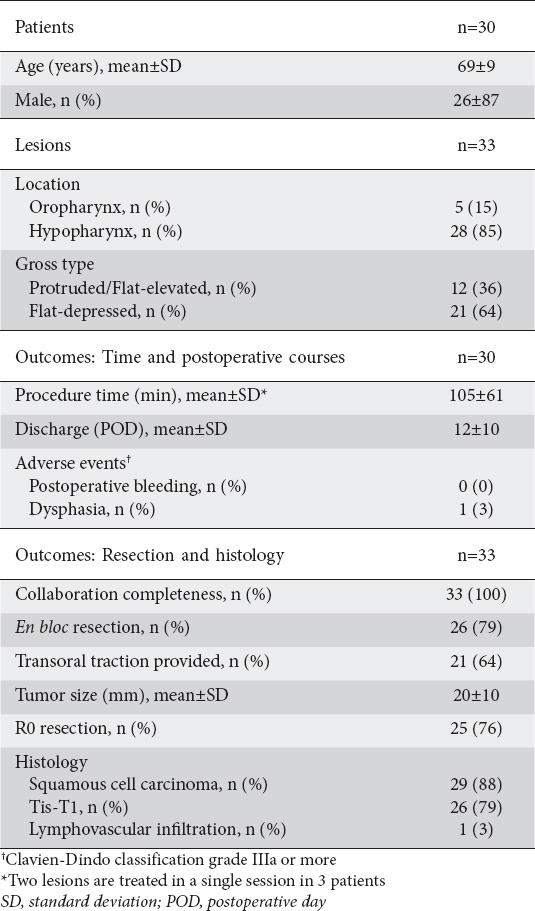
Results: Collaboration surgery was performed for 134 lesions (33 laryngopharyngeal, 2 esophageal, 89 gastric, 8 duodenal and 2 recto-anal) in 131 patients. Collaboration completeness was achieved in 129 lesions (96%). En bloc resection and pathological R0 resection of lesions were achieved in 127 (95%) and 124 (93%) lesions, respectively. The mean procedure time was 188 min. The mean time of discharge was the 11th postoperative day. Five patients (4%) developed relevant postoperative adverse events.
Conclusions: These results indicate that collaborative surgery by endoscopists and surgeons was feasible and safe, and may contribute to providing less invasive treatment than conventional surgery. Collaborative surgery is worth considering as a flexible and reliable surgical option, when cooperation may outperform either treatment alone.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


