Isaac G Freedman, Michael R Mercier, Anoop R Galivanche, Mani Ratnesh S Sandhu, Mark Hocevar, Harold Gregory Moore, Jonathan N Grauer, Lee E Rubin, Jinlei Li
{"title":"Continuous Adductor Canal Block Compared to Epidural Anesthesia for Total Knee Arthroplasty.","authors":"Isaac G Freedman, Michael R Mercier, Anoop R Galivanche, Mani Ratnesh S Sandhu, Mark Hocevar, Harold Gregory Moore, Jonathan N Grauer, Lee E Rubin, Jinlei Li","doi":"10.2147/JPR.S462079","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To compare the efficacy of a postoperative continuous adductor canal block (cACB) with and without a steroid adjuvant to that of epidural analgesia (EA).</p><p><strong>Methods: </strong>Patients who underwent primary total TKA at a single institution between July 2011-November 2017 were included for retrospective analysis. TKA patients were stratified into one of the three analgesia approaches: EA, cACB without steroid adjuvant, and cACB with steroid adjuvant. Hospital length of stay (LOS), discharge disposition, incidence of postoperative adverse events, and total milligram morphine equivalents (MME) requirements were compared between strata. Logistic regressions were performed to assess the independent effect of analgesia approach on prolonged LOS greater than 3 days (pLOS), non-home discharge, and total and daily MME requirements (tMME and dMME) following TKA.</p><p><strong>Results: </strong>Of the 4345 patients undergoing TKA, 1556 (35.83%) received EA, 2087 (48.03%) received cACB without steroids, and 702 (16.13%) cACB with steroids. cACB patients experienced lower rates of pLOS, higher rates of discharge to home than EA patients, and lower tMME and dMME. On multivariable analysis, cACB groups were at a lower odds of experiencing a pLOS compared to EA patients without steroids (OR = 0.64; 95% CI 0.49-0.84; with steroids: OR = 0.54; 95% CI 0.38-0.76). cACB groups had lower odds of a non-home discharge when compared to EA patients (without steroids OR = 0.42; 95% CI 0.36-0.48; with steroids: OR 0.22; 95% CI 0.18-0.27). On multivariable analysis, cACB groups required less tMME compared to the EA group (without steroids β=-290 mmE; 95% CI: -313 to -268 mmE; with steroids: β=-261 mmE; 95% CI: -289 to -233 mmE) as well as lower dMME (without steroids: β=-66 mmE/day; 95% CI -72 to -60 mmE/day; with steroids: β=-48 mmE/day; 95% CI -55 to -40 mmE/day).</p><p><strong>Conclusion: </strong>cACB was associated with greater discharge to home rates, lower rates of pLOS, and lower tMME and dMME consumption.</p><p><strong>Level of evidence: </strong>Level III.</p>","PeriodicalId":16661,"journal":{"name":"Journal of Pain Research","volume":"17 ","pages":"3729-3740"},"PeriodicalIF":2.5000,"publicationDate":"2024-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11572497/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pain Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JPR.S462079","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To compare the efficacy of a postoperative continuous adductor canal block (cACB) with and without a steroid adjuvant to that of epidural analgesia (EA).
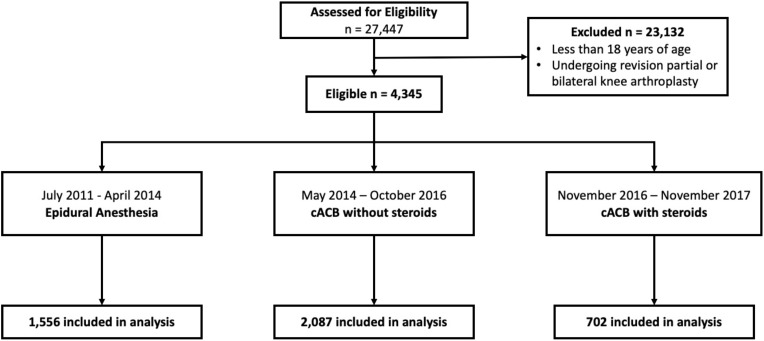
Methods: Patients who underwent primary total TKA at a single institution between July 2011-November 2017 were included for retrospective analysis. TKA patients were stratified into one of the three analgesia approaches: EA, cACB without steroid adjuvant, and cACB with steroid adjuvant. Hospital length of stay (LOS), discharge disposition, incidence of postoperative adverse events, and total milligram morphine equivalents (MME) requirements were compared between strata. Logistic regressions were performed to assess the independent effect of analgesia approach on prolonged LOS greater than 3 days (pLOS), non-home discharge, and total and daily MME requirements (tMME and dMME) following TKA.
Results: Of the 4345 patients undergoing TKA, 1556 (35.83%) received EA, 2087 (48.03%) received cACB without steroids, and 702 (16.13%) cACB with steroids. cACB patients experienced lower rates of pLOS, higher rates of discharge to home than EA patients, and lower tMME and dMME. On multivariable analysis, cACB groups were at a lower odds of experiencing a pLOS compared to EA patients without steroids (OR = 0.64; 95% CI 0.49-0.84; with steroids: OR = 0.54; 95% CI 0.38-0.76). cACB groups had lower odds of a non-home discharge when compared to EA patients (without steroids OR = 0.42; 95% CI 0.36-0.48; with steroids: OR 0.22; 95% CI 0.18-0.27). On multivariable analysis, cACB groups required less tMME compared to the EA group (without steroids β=-290 mmE; 95% CI: -313 to -268 mmE; with steroids: β=-261 mmE; 95% CI: -289 to -233 mmE) as well as lower dMME (without steroids: β=-66 mmE/day; 95% CI -72 to -60 mmE/day; with steroids: β=-48 mmE/day; 95% CI -55 to -40 mmE/day).
Conclusion: cACB was associated with greater discharge to home rates, lower rates of pLOS, and lower tMME and dMME consumption.
期刊介绍:
Journal of Pain Research is an international, peer-reviewed, open access journal that welcomes laboratory and clinical findings in the fields of pain research and the prevention and management of pain. Original research, reviews, symposium reports, hypothesis formation and commentaries are all considered for publication. Additionally, the journal now welcomes the submission of pain-policy-related editorials and commentaries, particularly in regard to ethical, regulatory, forensic, and other legal issues in pain medicine, and to the education of pain practitioners and researchers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


