Associations of physiologic subtypes based on HOMA2 indices of β-cell function and insulin sensitivity with the risk of kidney function decline, cardiovascular disease, and all-cause mortality from the 4C study.
{"title":"Associations of physiologic subtypes based on HOMA2 indices of β-cell function and insulin sensitivity with the risk of kidney function decline, cardiovascular disease, and all-cause mortality from the 4C study.","authors":"Peiqiong Luo, Danpei Li, Yaming Guo, Xiaoyu Meng, Ranran Kan, Limeng Pan, Yuxi Xiang, Beibei Mao, Yi He, Siyi Wang, Yan Yang, Zhelong Liu, Junhui Xie, Benping Zhang, Wentao He, Shuhong Hu, Xinrong Zhou, Xuefeng Yu","doi":"10.1186/s12933-024-02496-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous studies have been limited by their inability to differentiate between the effects of insulin sensitivity and β-cell function on the risk of kidney function decline, cardiovascular disease (CVD), and all-cause mortality. To address this knowledge gap, we aimed to investigate whether the physiological subtypes based on homeostasis model assessment-2 (HOMA2) indices of β-cell function (HOMA2-B) and insulin sensitivity (HOMA2-S) could be used to identify individuals with subsequently high or low of clinical outcome risk.</p><p><strong>Methods: </strong>This retrospective cohort study included 7,317 participants with a follow-up of up to 5 years. Based on HOMA2 indices, participants were categorized into four physiologic subtypes: the normal phenotype (high insulin sensitivity and high β-cell function), the insulinopenic phenotype (high insulin sensitivity and low β-cell function), the hyperinsulinaemic phenotype (low insulin sensitivity and high β-cell function), and the classical phenotype (low insulin sensitivity and low β-cell function). The outcomes included kidney function decline, CVD events (fatal and nonfatal), and all-cause mortality. Cox regression models were used to calculate hazard ratios (HRs) for outcomes, and spline models were used to examine the dose-dependent associations of HOMA2-B and HOMA2-S with outcomes.</p><p><strong>Results: </strong>A total of 1,488 (20.3%) were classified as normal, 2,179 (29.8%) as insulinopenic, 2,173 (29.7%) as hyperinsulinemic, and 1,477 (20.2%) as classical subtypes. Compared with other physiological subtypes, the classical subtype presented the highest risk of kidney function decline (classical vs. normal HR 11.50, 95% CI 4.31-30.67). The hyperinsulinemic subtype had the highest risk of CVD and all-cause mortality (hyperinsulinemic vs. normal: fatal CVD, HR 6.56, 95% CI 3.09-13.92; all-cause mortality, HR 4.56, 95% CI 2.97-7.00). Spline analyses indicated the dose-dependent associations of HOMA2-B and HOMA2-S with outcomes.</p><p><strong>Conclusions: </strong>The classical subtype had the strongest correlation with the risk of kidney function decline, and the hyperinsulinemic subtype had the highest risk of CVD and all-cause mortality, which should be considered for interventions with precision medicine.</p>","PeriodicalId":9374,"journal":{"name":"Cardiovascular Diabetology","volume":"23 1","pages":"401"},"PeriodicalIF":10.6000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11546320/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Diabetology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12933-024-02496-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Previous studies have been limited by their inability to differentiate between the effects of insulin sensitivity and β-cell function on the risk of kidney function decline, cardiovascular disease (CVD), and all-cause mortality. To address this knowledge gap, we aimed to investigate whether the physiological subtypes based on homeostasis model assessment-2 (HOMA2) indices of β-cell function (HOMA2-B) and insulin sensitivity (HOMA2-S) could be used to identify individuals with subsequently high or low of clinical outcome risk.
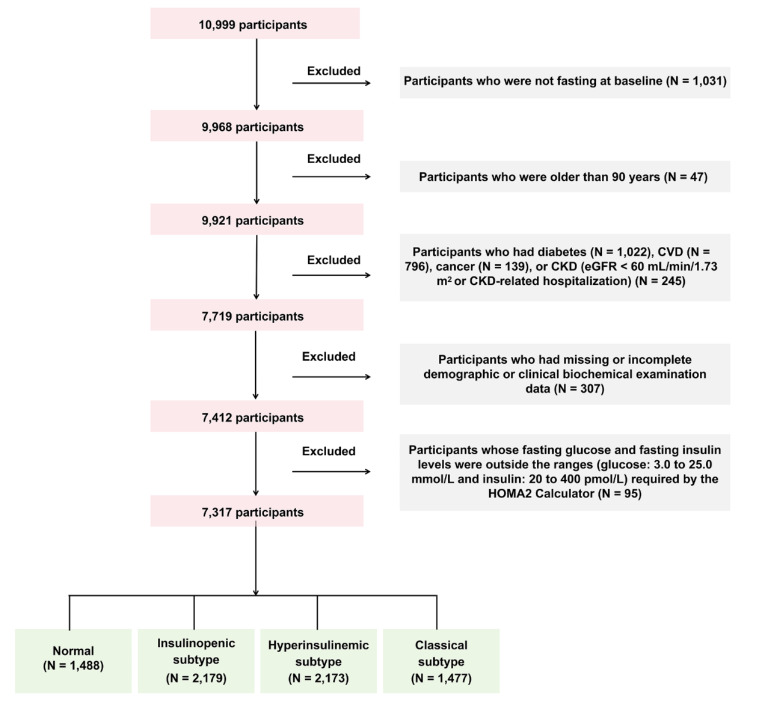
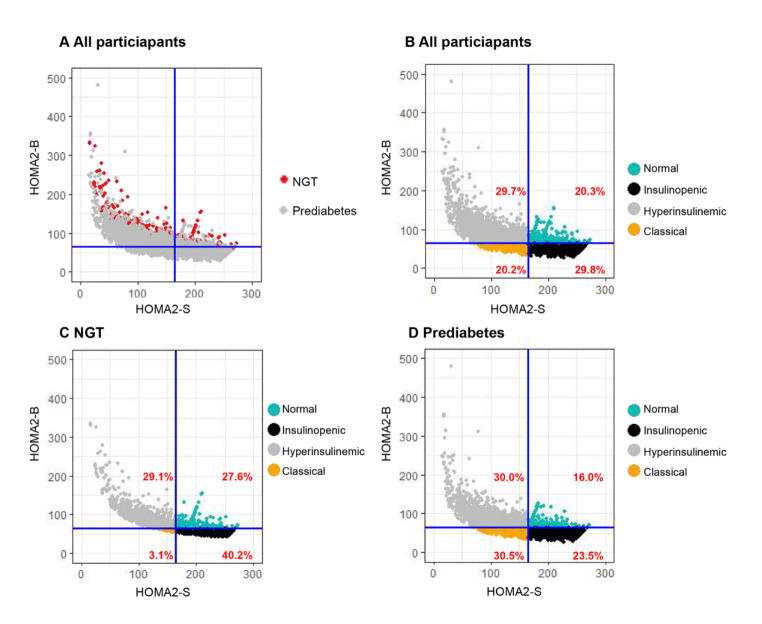
Methods: This retrospective cohort study included 7,317 participants with a follow-up of up to 5 years. Based on HOMA2 indices, participants were categorized into four physiologic subtypes: the normal phenotype (high insulin sensitivity and high β-cell function), the insulinopenic phenotype (high insulin sensitivity and low β-cell function), the hyperinsulinaemic phenotype (low insulin sensitivity and high β-cell function), and the classical phenotype (low insulin sensitivity and low β-cell function). The outcomes included kidney function decline, CVD events (fatal and nonfatal), and all-cause mortality. Cox regression models were used to calculate hazard ratios (HRs) for outcomes, and spline models were used to examine the dose-dependent associations of HOMA2-B and HOMA2-S with outcomes.
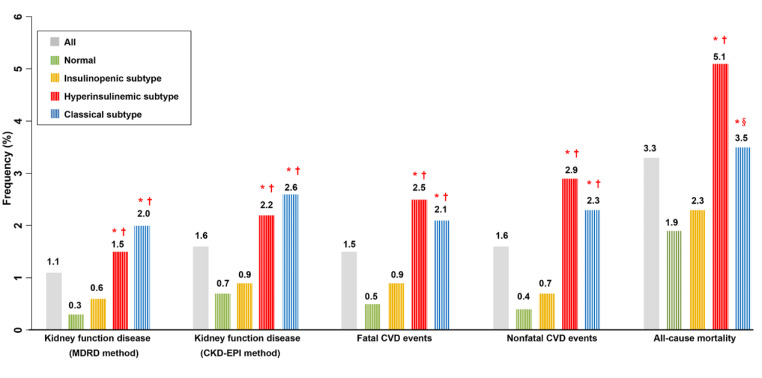
Results: A total of 1,488 (20.3%) were classified as normal, 2,179 (29.8%) as insulinopenic, 2,173 (29.7%) as hyperinsulinemic, and 1,477 (20.2%) as classical subtypes. Compared with other physiological subtypes, the classical subtype presented the highest risk of kidney function decline (classical vs. normal HR 11.50, 95% CI 4.31-30.67). The hyperinsulinemic subtype had the highest risk of CVD and all-cause mortality (hyperinsulinemic vs. normal: fatal CVD, HR 6.56, 95% CI 3.09-13.92; all-cause mortality, HR 4.56, 95% CI 2.97-7.00). Spline analyses indicated the dose-dependent associations of HOMA2-B and HOMA2-S with outcomes.
Conclusions: The classical subtype had the strongest correlation with the risk of kidney function decline, and the hyperinsulinemic subtype had the highest risk of CVD and all-cause mortality, which should be considered for interventions with precision medicine.
期刊介绍:
Cardiovascular Diabetology is a journal that welcomes manuscripts exploring various aspects of the relationship between diabetes, cardiovascular health, and the metabolic syndrome. We invite submissions related to clinical studies, genetic investigations, experimental research, pharmacological studies, epidemiological analyses, and molecular biology research in this field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


