Sex Differences in Outcomes of Adults with Repaired Coarctation of Aorta and Concomitant Aortic Valve Disease
IF 2.5
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
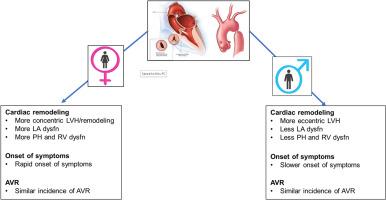
Aortic valve disease is common in adults with coarctation of aorta. However, no systematic comparative analyses have been performed of the clinical course of aortic valve disease for male vs female patients in this population. The purpose of this study was to compare cardiac remodelling, onset of symptoms, and incidence of aortic valve replacement (AVR) for male vs female patients.
Methods
A retrospective study was conducted of adults with repaired coarctation of aorta and ≥ moderate aortic stenosis and/or aortic regurgitation. Cardiac remodelling (left ventricular [LV], left atrial, right ventricular [RV], and right atrial structure and function) and symptomatic and/or functional class were determined at the baseline encounter. Development of new-onset symptoms and the incidence of AVR were ascertained for the period from baseline to last encounter.
Results
We identified 214 patients (121 male [57%], 93 female [43%]). Although both groups had a similar aortic valve gradient, aortic valve area indexed to body surface area, aortic regurgitation severity, and functional status at baseline, female patients had more LV concentric hypertrophy and remodelling, left atrial hypertension and dysfunction, elevated RV systolic pressure, and RV systolic dysfunction. Of 151 patients without symptoms at baseline,102 (72%) developed symptoms. Female sex was independently associated with new-onset symptoms (adjusted hazard ratio 1.14, [95% confidence interval 1.05-1.23]). Of 214 patients, 191 (89%) underwent AVR. Female sex was not associated with AVR upon multivariable analysis. However, LV concentric hypertrophy and remodelling (both of which were more common in female patients) were associated with new-onset symptoms and AVR.
Conclusions
Female patients, compared to male patients, had more-advanced cardiac remodelling, and more-rapid onset of symptoms, but a similar risk of AVR.
主动脉瓣修复后并发主动脉瓣病变的成人预后的性别差异
背景主动脉瓣疾病在患有主动脉共动脉症的成人中很常见。然而,目前还没有对这一人群中男性和女性主动脉瓣疾病的临床过程进行系统的比较分析。本研究的目的是比较男性和女性患者的心脏重塑、症状出现和主动脉瓣置换术(AVR)的发生率。方法对主动脉副截管修复后主动脉瓣瓣膜≥中度狭窄和/或主动脉瓣反流的成人进行回顾性研究。在基线检查时确定心脏重塑(左心室、左心房、右心室和右心房的结构和功能)以及症状和/或功能分级。结果我们发现了 214 名患者(121 名男性[57%],93 名女性[43%])。虽然两组患者的主动脉瓣梯度、主动脉瓣面积与体表面积的指数、主动脉瓣反流严重程度和基线时的功能状态相似,但女性患者的左心室同心度肥大和重构、左心房高血压和功能障碍、RV 收缩压升高和 RV 收缩功能障碍更多。在基线时无症状的 151 名患者中,102 人(72%)出现了症状。女性性别与新发症状独立相关(调整后危险比为 1.14,[95% 置信区间为 1.05-1.23])。在 214 名患者中,191 人(89%)接受了房室重建术。经多变量分析,女性性别与房室重建无关。然而,左心室同心度肥大和重塑(这两种情况在女性患者中更为常见)与新发症状和房室重建相关。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

CJC Open
Medicine-Cardiology and Cardiovascular Medicine
CiteScore
3.30
自引率
0.00%
发文量
143
审稿时长
60 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


