Jeffrey K Belkora, Jill Reichert, Katherine Williams, Mary A Whooley, Talayeh Rezayat, Stacy Sorensen, Priyanka Chilakamarri, Elizabeth Sanders, Andrea Maas, Alexander Gomez, Philip Kurien, Liza Ashbrook, Jacque Thomas, Kathleen F Sarmiento
{"title":"Implementing TeleSleep at Veterans Healthcare Administration: an organizational case study of adaptation and sustainment.","authors":"Jeffrey K Belkora, Jill Reichert, Katherine Williams, Mary A Whooley, Talayeh Rezayat, Stacy Sorensen, Priyanka Chilakamarri, Elizabeth Sanders, Andrea Maas, Alexander Gomez, Philip Kurien, Liza Ashbrook, Jacque Thomas, Kathleen F Sarmiento","doi":"10.3389/frsle.2024.1444689","DOIUrl":null,"url":null,"abstract":"<p><p>Veteran access to sleep medicine is of paramount importance to the Veterans Health Administration (VA). To increase access, VA has created community referral policies and programs, as well as telehealth programs. In 2017, the Office of Rural Health (ORH) funded a TeleSleep initiative focused on reaching rural Veterans with unmet sleep needs. ORH provided 3-6 years of funding to help 19 hubs support 98 spoke sites serving rural Veterans. As ORH funding concluded, each hub identified its path to sustainment. This case study follows one TeleSleep hub in VA's western geographic region as it transitioned from ORH funding sustainment as a regional Sleep Clinical Resource Hub. This case study describes the real-world process of adaptation in care delivery strategies. One key area of adaptation revolved around whether to deliver care via the patient's home facility or the provider's home facility. In early 2021, the TeleSleep team implemented an innovative provider transfer model, where temporary reinforcements from the TeleSleep hub increased the workforce capacity of spoke sites, similar to the concept of locum tenens. In this provider transfer model, TeleSleep clinicians scheduled, documented, and billed for each encounter at the Veteran's home facility. Positioning TeleSleep clinicians as local providers facilitated communication and referrals and promoted continuity and quality of care for Veterans in their home facility. This provider transfer model reduced the administrative burden of providers and schedulers and supported patient-side-only documentation of care. While this mirrors current locum tenens practice, transferring providers did not fit VA's financial model as implemented by the western region's Sleep Clinical Resource Hub. Therefore, in December 2021, VA aligned TeleSleep with VA's preferred practice of patient rather than provider transfers. In the patient transfer model, providers schedule and document in both the provider and patient electronic health records, and bill in the provider's facility. However, reflecting on this period of innovation, TeleSleep team members concluded that the provider transfer model could improve patient safety and care coordination while reducing the administrative burden of frontline clinicians. Further research and development are needed to align the provider transfer model with VA's financial model.</p>","PeriodicalId":73106,"journal":{"name":"Frontiers in sleep","volume":"3 ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11539190/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in sleep","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/frsle.2024.1444689","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
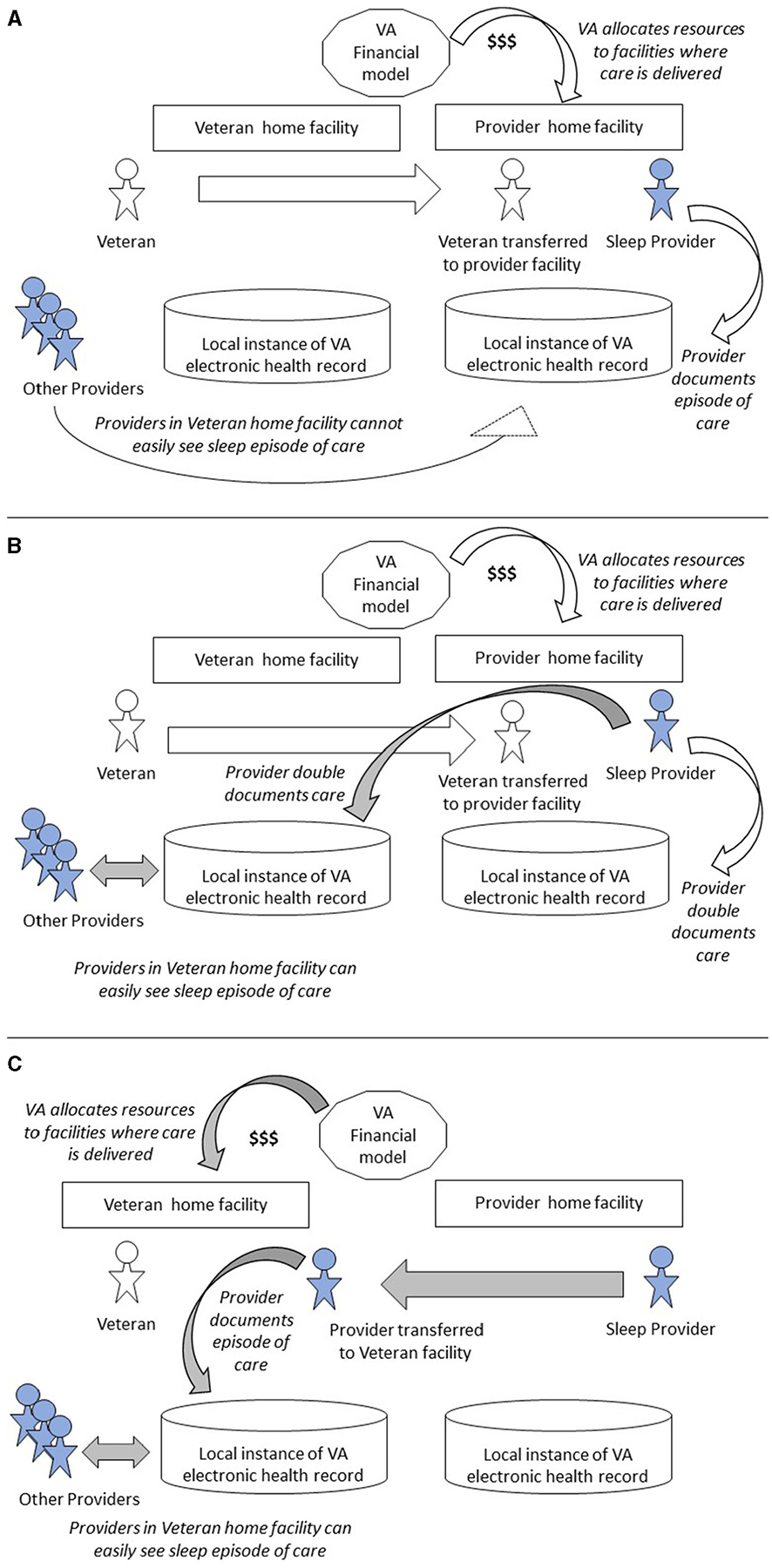
Veteran access to sleep medicine is of paramount importance to the Veterans Health Administration (VA). To increase access, VA has created community referral policies and programs, as well as telehealth programs. In 2017, the Office of Rural Health (ORH) funded a TeleSleep initiative focused on reaching rural Veterans with unmet sleep needs. ORH provided 3-6 years of funding to help 19 hubs support 98 spoke sites serving rural Veterans. As ORH funding concluded, each hub identified its path to sustainment. This case study follows one TeleSleep hub in VA's western geographic region as it transitioned from ORH funding sustainment as a regional Sleep Clinical Resource Hub. This case study describes the real-world process of adaptation in care delivery strategies. One key area of adaptation revolved around whether to deliver care via the patient's home facility or the provider's home facility. In early 2021, the TeleSleep team implemented an innovative provider transfer model, where temporary reinforcements from the TeleSleep hub increased the workforce capacity of spoke sites, similar to the concept of locum tenens. In this provider transfer model, TeleSleep clinicians scheduled, documented, and billed for each encounter at the Veteran's home facility. Positioning TeleSleep clinicians as local providers facilitated communication and referrals and promoted continuity and quality of care for Veterans in their home facility. This provider transfer model reduced the administrative burden of providers and schedulers and supported patient-side-only documentation of care. While this mirrors current locum tenens practice, transferring providers did not fit VA's financial model as implemented by the western region's Sleep Clinical Resource Hub. Therefore, in December 2021, VA aligned TeleSleep with VA's preferred practice of patient rather than provider transfers. In the patient transfer model, providers schedule and document in both the provider and patient electronic health records, and bill in the provider's facility. However, reflecting on this period of innovation, TeleSleep team members concluded that the provider transfer model could improve patient safety and care coordination while reducing the administrative burden of frontline clinicians. Further research and development are needed to align the provider transfer model with VA's financial model.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


