Andreia Cardoso, Sara Anacleto, Catarina Laranjo Tinoco, Ana Sofia Araújo, Mariana Capinha, Luís Borges Pinto, Aparício Coutinho, Catarina Tavares, Vera Marques, Paulo Mota, Miguel Mendes, Carlos Oliveira, João Pimentel Torres, Emanuel Carvalho-Dias
{"title":"\"Minho Technique\" for Laparoscopic Radical Cystectomy with Intracorporeal Ileal Conduit.","authors":"Andreia Cardoso, Sara Anacleto, Catarina Laranjo Tinoco, Ana Sofia Araújo, Mariana Capinha, Luís Borges Pinto, Aparício Coutinho, Catarina Tavares, Vera Marques, Paulo Mota, Miguel Mendes, Carlos Oliveira, João Pimentel Torres, Emanuel Carvalho-Dias","doi":"10.5152/tud.2024.23230","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Radical cystectomy (RC) with ileal conduit (IC) remains a main treatment for muscle-invasive bladder cancer (MIBC). Laparoscopy in this multistage surgery is quite demanding, so laparoscopic RC (LRC) with intracorporeal IC (IIC) is a technically exceptional procedure. We aim to simplify it, demonstrating our technique, step-by-step. We present a 4-port LRC with IIC and Bricker uretero-ileal anastomoses. The main difference is the immediate and complete posterior dissection, similar to the \"Montsouris approach\" for prostatectomy.</p><p><strong>Materials and methods: </strong>A 70-year-old man with a 5 cm MIBC was subjected to our demonstrated procedure.</p><p><strong>Results: </strong>The postoperative period was uneventful. Diet and ambulation: 2 days. Single-J stents removal: 4 weeks. MIBC N0 was confirmed. At 24 months, the patient is well, without complications (namely hydronephrosis or disease recurrence).</p><p><strong>Conclusion: </strong>LRC with IIC is demanding and requires laparoscopic expertise. However, if performed in a standardized fashion, as demonstrated through this case, and considering our center's experience, it seems feasible and safe with 4-port and standard material without a significant operative time increase, nor oncological or functional compromise.</p>","PeriodicalId":101337,"journal":{"name":"Urology research & practice","volume":"50 3","pages":"203-207"},"PeriodicalIF":1.1000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11562924/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urology research & practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/tud.2024.23230","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
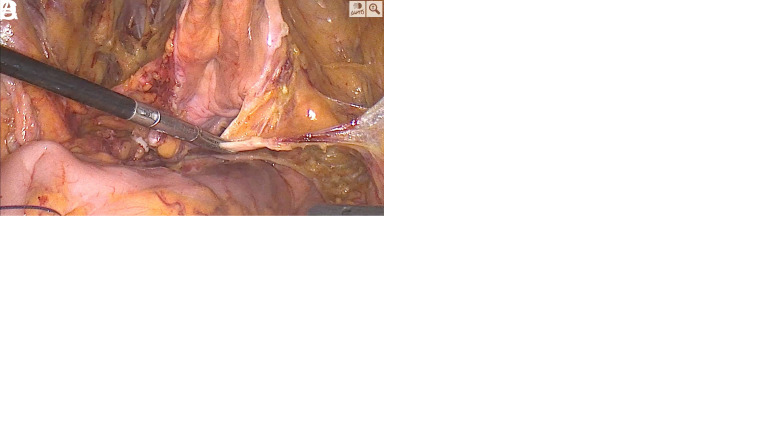
Objective: Radical cystectomy (RC) with ileal conduit (IC) remains a main treatment for muscle-invasive bladder cancer (MIBC). Laparoscopy in this multistage surgery is quite demanding, so laparoscopic RC (LRC) with intracorporeal IC (IIC) is a technically exceptional procedure. We aim to simplify it, demonstrating our technique, step-by-step. We present a 4-port LRC with IIC and Bricker uretero-ileal anastomoses. The main difference is the immediate and complete posterior dissection, similar to the "Montsouris approach" for prostatectomy.
Materials and methods: A 70-year-old man with a 5 cm MIBC was subjected to our demonstrated procedure.
Results: The postoperative period was uneventful. Diet and ambulation: 2 days. Single-J stents removal: 4 weeks. MIBC N0 was confirmed. At 24 months, the patient is well, without complications (namely hydronephrosis or disease recurrence).
Conclusion: LRC with IIC is demanding and requires laparoscopic expertise. However, if performed in a standardized fashion, as demonstrated through this case, and considering our center's experience, it seems feasible and safe with 4-port and standard material without a significant operative time increase, nor oncological or functional compromise.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


