Ning Jiao, Cheng Yan, Li He, Hai-Long Jin, Shuang Oiu, Chao Li, Zhi-Sheng Zheng, Bin Lu, Feng-Dong Wu, Yang Yang, Xin-Guo Chen, Qing Zhang
{"title":"Liver transplantation for hepatocellular carcinoma: a proposal for including preoperative serological indicators improves the Milan criteria expanded.","authors":"Ning Jiao, Cheng Yan, Li He, Hai-Long Jin, Shuang Oiu, Chao Li, Zhi-Sheng Zheng, Bin Lu, Feng-Dong Wu, Yang Yang, Xin-Guo Chen, Qing Zhang","doi":"10.21037/tgh-24-40","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Liver transplantation (LT) is the most effective and radical treatment for hepatocellular carcinoma (HCC). Most LT criteria are based on the morphological characteristics of tumors, which are not enough to predict the risk of tumor recurrence. It is found that some serological biomarkers can predict tumor recurrence and may be a good indicator for selecting suitable HCC patients for LT. This article aims to evaluate the predictive effect of preoperative serological indicators on long-term overall survival (OS) and tumor recurrence-free survival (TFS) of patients with HCC after LT, and to explore its significance for expanding the Milan criteria.</p><p><strong>Methods: </strong>Clinical data of 253 patients after LT in HCC were collected retrospectively. The receiver operating characteristic curve was used to calculate the best cut-off value. χ<sup>2</sup> test was used to analyze the correlation between preoperative serological indicators and tumor pathological features. Univariate and multivariate analyses were used to analyze the risk factors affecting the OS and TFS rates and the predictive values of different LT criteria were compared. Nomogram model was used to predict the OS and TFS rates of patients exceeding Milan criteria.</p><p><strong>Results: </strong>Independent risk factors for poor OS and TFS rates were alpha-fetoprotein (AFP) >200 ng/mL, gamma-glutamyl transpeptidase (GGT) >80 IU/L, total tumor diameter (TTD) >8 cm and microsatellite lesions. Nomogram model showed patients beyond Milan criteria had better survival when AFP ≤200 ng/mL and GGT ≤80 IU/L or AFP >200 ng/mL, GGT ≤80 IU/L and TTD ≤8 cm. According to Milan criteria, AFP, GGT and TTD, Milan-AFP-GGT-TTD (M-AGT) criteria was established. There was no significant difference in OS and TFS rates among patients in M-AGT, Milan, Hangzhou, Malaya and the University of California at San Francisco (UCSF) criteria.</p><p><strong>Conclusions: </strong>Preoperative serological indicators AFP and GGT can effectively predict long-term OS and TFS in HCC patients after LT. Establishing M-AGT criteria based on serological indicators is helpful to supplement the Milan criteria.</p>","PeriodicalId":94362,"journal":{"name":"Translational gastroenterology and hepatology","volume":"9 ","pages":"63"},"PeriodicalIF":2.5000,"publicationDate":"2024-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11535812/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/tgh-24-40","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Liver transplantation (LT) is the most effective and radical treatment for hepatocellular carcinoma (HCC). Most LT criteria are based on the morphological characteristics of tumors, which are not enough to predict the risk of tumor recurrence. It is found that some serological biomarkers can predict tumor recurrence and may be a good indicator for selecting suitable HCC patients for LT. This article aims to evaluate the predictive effect of preoperative serological indicators on long-term overall survival (OS) and tumor recurrence-free survival (TFS) of patients with HCC after LT, and to explore its significance for expanding the Milan criteria.
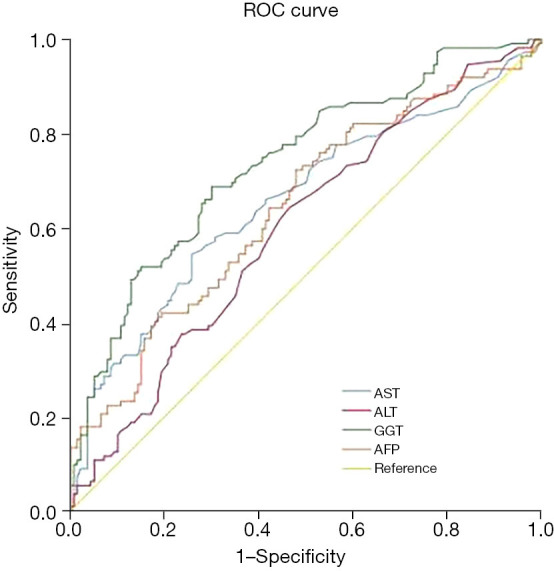
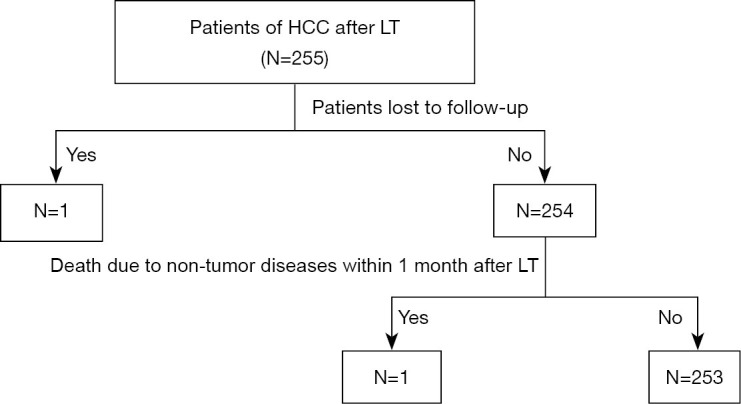
Methods: Clinical data of 253 patients after LT in HCC were collected retrospectively. The receiver operating characteristic curve was used to calculate the best cut-off value. χ2 test was used to analyze the correlation between preoperative serological indicators and tumor pathological features. Univariate and multivariate analyses were used to analyze the risk factors affecting the OS and TFS rates and the predictive values of different LT criteria were compared. Nomogram model was used to predict the OS and TFS rates of patients exceeding Milan criteria.
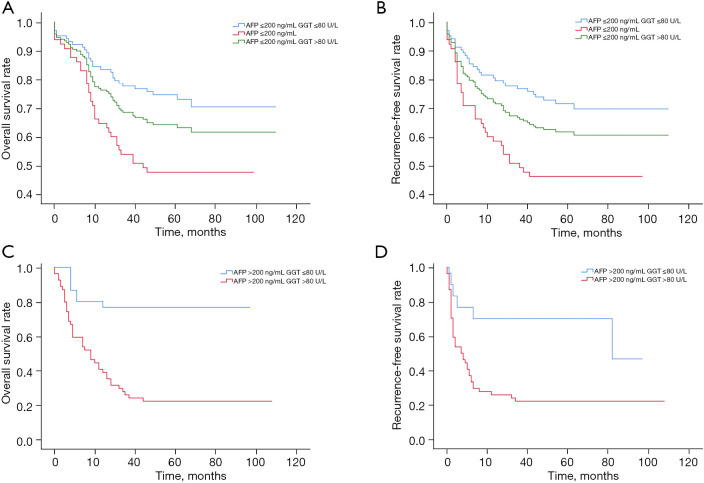
Results: Independent risk factors for poor OS and TFS rates were alpha-fetoprotein (AFP) >200 ng/mL, gamma-glutamyl transpeptidase (GGT) >80 IU/L, total tumor diameter (TTD) >8 cm and microsatellite lesions. Nomogram model showed patients beyond Milan criteria had better survival when AFP ≤200 ng/mL and GGT ≤80 IU/L or AFP >200 ng/mL, GGT ≤80 IU/L and TTD ≤8 cm. According to Milan criteria, AFP, GGT and TTD, Milan-AFP-GGT-TTD (M-AGT) criteria was established. There was no significant difference in OS and TFS rates among patients in M-AGT, Milan, Hangzhou, Malaya and the University of California at San Francisco (UCSF) criteria.
Conclusions: Preoperative serological indicators AFP and GGT can effectively predict long-term OS and TFS in HCC patients after LT. Establishing M-AGT criteria based on serological indicators is helpful to supplement the Milan criteria.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


