{"title":"Short-term severe polyuria responsive to vasopressin after hypoglycaemia and hypotension in a domestic shorthair cat.","authors":"Federica Porcarelli, Carla Asorey Blazquez, Ferran Valls Sanchez, Elena Scarpante, Giacomo Stanzani","doi":"10.1177/20551169241283294","DOIUrl":null,"url":null,"abstract":"<p><strong>Case summary: </strong>An 8-month-old male neutered domestic shorthair cat presented for acute vomiting. Abdominal ultrasound examination revealed a jejunal foreign body, which was removed via enterotomy. Preoperatively, the patient was hypoglycaemic and, intraoperatively, a dopamine infusion was required to maintain a mean arterial pressure >60 mmHg. Despite glucose supplementation, the cat remained severely hypoglycaemic on recovery. Within 24 h postoperatively, despite euglycaemia and normalisation of the cardiovascular status, the patient developed progressive polyuria (up to 14 ml/kg/h). This was associated with neurological signs suggestive of diffuse brain disease, and absence of azotaemia or signs of overhydration. During the first 4 days of hospitalisation, any attempts to decrease intravenous fluid therapy were associated with hypotension, weight loss and clinical dehydration. Urine specific gravity (USG) during this time was in the range of 1.005-1.010 and failed to increase during fluid challenges. A presumptive diagnosis of central diabetes insipidus was made, and desmopressin (1 µg/cat SC) was administered on day 5 of hospitalisation. Consequently, the cat's urinary output decreased and his weight increased within 4 h. The patient required a total of four doses of desmopressin during hospitalisation, but no further doses since discharge. Urinary output on discharge was 3 ml/kg/h. Three months later, the cat's neurological signs and polyuria had completely resolved, and the USG was >1.050.</p><p><strong>Relevance and novel information: </strong>In this case, a presumptive diagnosis of central diabetes insipidus was supported by clinical progression, neurological signs and the response to desmopressin. To our knowledge, this is the first report of reversible diabetes insipidus after diffuse brain injury secondary to hypotension and hypoglycaemia.</p>","PeriodicalId":36588,"journal":{"name":"Journal of Feline Medicine and Surgery Open Reports","volume":"10 2","pages":"20551169241283294"},"PeriodicalIF":0.7000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11536369/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Feline Medicine and Surgery Open Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20551169241283294","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
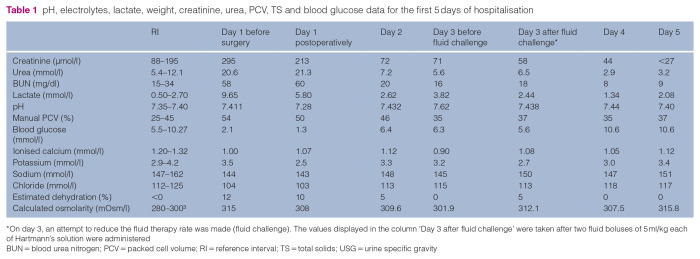
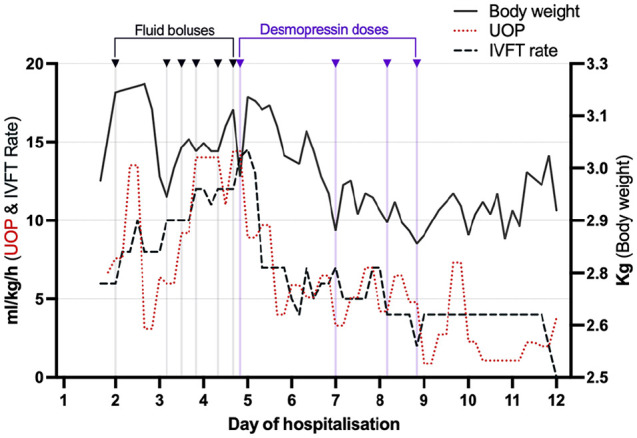
Case summary: An 8-month-old male neutered domestic shorthair cat presented for acute vomiting. Abdominal ultrasound examination revealed a jejunal foreign body, which was removed via enterotomy. Preoperatively, the patient was hypoglycaemic and, intraoperatively, a dopamine infusion was required to maintain a mean arterial pressure >60 mmHg. Despite glucose supplementation, the cat remained severely hypoglycaemic on recovery. Within 24 h postoperatively, despite euglycaemia and normalisation of the cardiovascular status, the patient developed progressive polyuria (up to 14 ml/kg/h). This was associated with neurological signs suggestive of diffuse brain disease, and absence of azotaemia or signs of overhydration. During the first 4 days of hospitalisation, any attempts to decrease intravenous fluid therapy were associated with hypotension, weight loss and clinical dehydration. Urine specific gravity (USG) during this time was in the range of 1.005-1.010 and failed to increase during fluid challenges. A presumptive diagnosis of central diabetes insipidus was made, and desmopressin (1 µg/cat SC) was administered on day 5 of hospitalisation. Consequently, the cat's urinary output decreased and his weight increased within 4 h. The patient required a total of four doses of desmopressin during hospitalisation, but no further doses since discharge. Urinary output on discharge was 3 ml/kg/h. Three months later, the cat's neurological signs and polyuria had completely resolved, and the USG was >1.050.
Relevance and novel information: In this case, a presumptive diagnosis of central diabetes insipidus was supported by clinical progression, neurological signs and the response to desmopressin. To our knowledge, this is the first report of reversible diabetes insipidus after diffuse brain injury secondary to hypotension and hypoglycaemia.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


