Sherry Erian, Rachelle Davies, Kylie Morrison, Christina West, Maria Ruiz, Iwona Zubik, Julie Nhan, Stephanie Thompson
{"title":"Increasing Accessibility to Intradialytic Cycling in Rural and Remote Settings: Program Report.","authors":"Sherry Erian, Rachelle Davies, Kylie Morrison, Christina West, Maria Ruiz, Iwona Zubik, Julie Nhan, Stephanie Thompson","doi":"10.1177/20543581241287591","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of program: </strong>Access to exercise and rehabilitation is often lower in rural or remote areas and hemodialysis (HD) dependence imposes additional barriers. Intradialytic cycling (IDC) can improve HD-related symptoms, such as leg cramping, restless legs, and symptoms of depression, as well as physical function and fitness, but access to exercise professionals with this expertise is limited. To promote access to IDC in rural and remote HD units, we describe the implementation and initial evaluation of a novel IDC program using virtual assessment to safely prescribe and individualize IDC.</p><p><strong>Sources of information: </strong>We developed and piloted a protocol for virtual IDC assessment and prospectively collected metrics informed by the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework to support future quality improvement activities.</p><p><strong>Methods: </strong>Rural HD units were defined as per Alberta Kidney Care North (AKC-N)'s operations. The virtual IDC program components were: HD unit education sessions, support and interest from local unit staff and those receiving HD, a bike, a supervising kinesiologist, a stable Internet connection, a nurse present during the 25-minute initial virtual assessment, and virtual follow-up every 3 to 4 weeks with the kinesiologist. The initial assessment consists of a virtual bike test where the participant performs a graded, symptom-limited cycling trial with documentation of vital signs and rating of self-perceived exertion (relative intensity). The data are used to prescribe IDC (frequency, intensity, time). The HD unit staff learn participant and bike set-up, confirm safe exercise parameters for that day, adjust the bike intensity, and take vital signs. Outcomes for evaluating the impact of the IDC program using the RE-AIM health framework were selected.</p><p><strong>Key findings: </strong>Out of the 24 HD units in AKC-N, 18 units were defined as either remote or rural (75%). Four of the units (22%) adopted the program, which was less than our target of 30% of units. Individual-level participation (Reach) within those units ranged widely (1-67%) with only one unit reaching the target of at least 30% individual-level participation. Reasons for starting IDC were intradialytic cramping, restless legs, deconditioning, and boredom during HD. Reasons for non-participation were lack of interest and a desire to sleep. Routine exercise program questionnaires on health-related quality of life for program effectiveness were not consistently completed by participants. All virtual assessments were completed as per protocol with a nurse (100% fidelity); however, tests often needed to be re-scheduled due to technical issues with Wi-Fi, limited unit staffing, operational demands, and/or safety concerns. At 1 year, all 4 units continued to participate with 2 additional HD units starting the following year.</p><p><strong>Limitations: </strong>Reach could be improved by introducing intradialytic exercise to individuals at HD initiation, prior to moving to their local satellite HD unit. Existing measures of program effectiveness may not be relevant to program participants or feasible to implement without an on-site exercise professional. Technical issues and navigating the busy schedules of unit staff were limitations to completing tests as scheduled.</p><p><strong>Implications: </strong>Implementing a protocolized approach with virtual support can increase accessibility to an evidence-based treatment in HD units without exercise professionals. For people requiring HD, reach may be improved with early education and exposure at HD start and with orientation sessions for staff. Adding a virtual IDC assessment day for staff as part of their routine monthly task schedule may promote institutionalization. Formalized follow-up sessions for kinesiologists and nurses to discuss program concerns would benefit the program in the future. Completion of program effectiveness measures may be improved by selecting more individualized options, for example, person-reported measures related to the individual's reason for referral.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241287591"},"PeriodicalIF":1.5000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11526228/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241287591","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose of program: Access to exercise and rehabilitation is often lower in rural or remote areas and hemodialysis (HD) dependence imposes additional barriers. Intradialytic cycling (IDC) can improve HD-related symptoms, such as leg cramping, restless legs, and symptoms of depression, as well as physical function and fitness, but access to exercise professionals with this expertise is limited. To promote access to IDC in rural and remote HD units, we describe the implementation and initial evaluation of a novel IDC program using virtual assessment to safely prescribe and individualize IDC.
Sources of information: We developed and piloted a protocol for virtual IDC assessment and prospectively collected metrics informed by the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework to support future quality improvement activities.
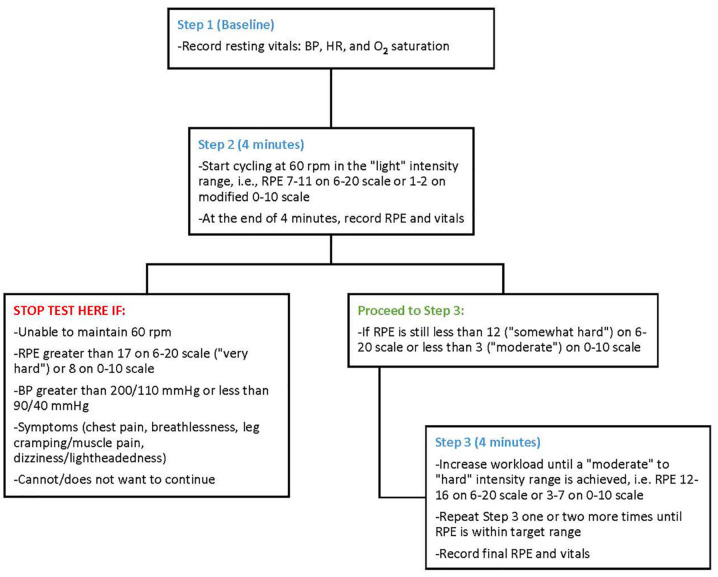
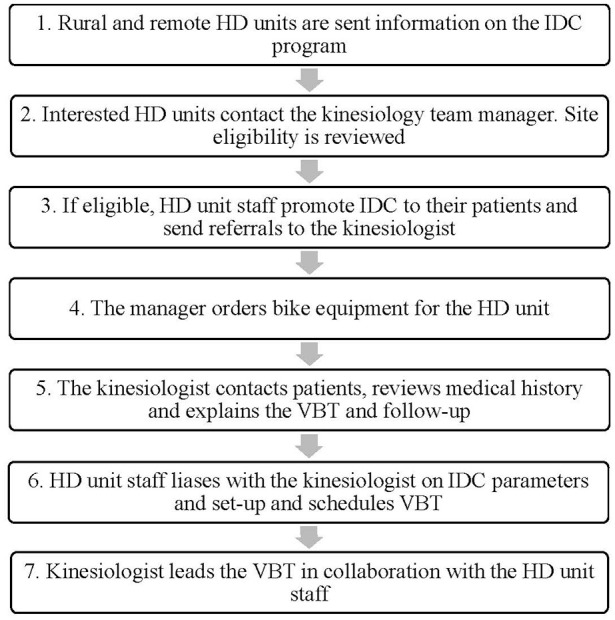
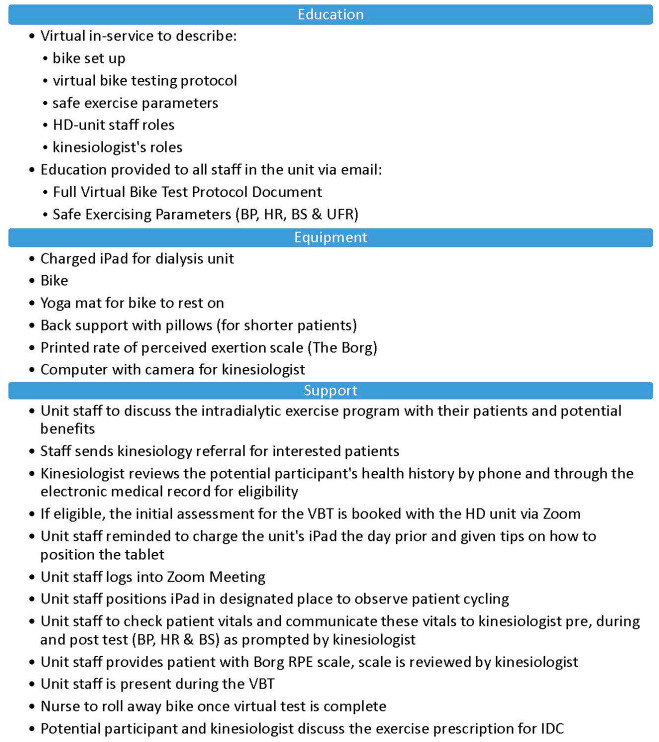
Methods: Rural HD units were defined as per Alberta Kidney Care North (AKC-N)'s operations. The virtual IDC program components were: HD unit education sessions, support and interest from local unit staff and those receiving HD, a bike, a supervising kinesiologist, a stable Internet connection, a nurse present during the 25-minute initial virtual assessment, and virtual follow-up every 3 to 4 weeks with the kinesiologist. The initial assessment consists of a virtual bike test where the participant performs a graded, symptom-limited cycling trial with documentation of vital signs and rating of self-perceived exertion (relative intensity). The data are used to prescribe IDC (frequency, intensity, time). The HD unit staff learn participant and bike set-up, confirm safe exercise parameters for that day, adjust the bike intensity, and take vital signs. Outcomes for evaluating the impact of the IDC program using the RE-AIM health framework were selected.
Key findings: Out of the 24 HD units in AKC-N, 18 units were defined as either remote or rural (75%). Four of the units (22%) adopted the program, which was less than our target of 30% of units. Individual-level participation (Reach) within those units ranged widely (1-67%) with only one unit reaching the target of at least 30% individual-level participation. Reasons for starting IDC were intradialytic cramping, restless legs, deconditioning, and boredom during HD. Reasons for non-participation were lack of interest and a desire to sleep. Routine exercise program questionnaires on health-related quality of life for program effectiveness were not consistently completed by participants. All virtual assessments were completed as per protocol with a nurse (100% fidelity); however, tests often needed to be re-scheduled due to technical issues with Wi-Fi, limited unit staffing, operational demands, and/or safety concerns. At 1 year, all 4 units continued to participate with 2 additional HD units starting the following year.
Limitations: Reach could be improved by introducing intradialytic exercise to individuals at HD initiation, prior to moving to their local satellite HD unit. Existing measures of program effectiveness may not be relevant to program participants or feasible to implement without an on-site exercise professional. Technical issues and navigating the busy schedules of unit staff were limitations to completing tests as scheduled.
Implications: Implementing a protocolized approach with virtual support can increase accessibility to an evidence-based treatment in HD units without exercise professionals. For people requiring HD, reach may be improved with early education and exposure at HD start and with orientation sessions for staff. Adding a virtual IDC assessment day for staff as part of their routine monthly task schedule may promote institutionalization. Formalized follow-up sessions for kinesiologists and nurses to discuss program concerns would benefit the program in the future. Completion of program effectiveness measures may be improved by selecting more individualized options, for example, person-reported measures related to the individual's reason for referral.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


