Reduced intestinal-to-diffuse conversion and immunosuppressive responses underlie superiority of neoadjuvant immunochemotherapy in gastric adenocarcinoma
{"title":"Reduced intestinal-to-diffuse conversion and immunosuppressive responses underlie superiority of neoadjuvant immunochemotherapy in gastric adenocarcinoma","authors":"Lei Wang, Linghong Wan, Xu Chen, Peng Gao, Yongying Hou, Linyu Wu, Wenkang Liu, Shuoran Tian, Mengyi Han, Shiyin Peng, Yuting Tan, Yuwei Pan, Yuanfeng Ren, Jinyang Li, Haihui Wen, Qin Liu, Mengsi Zhang, Tao Wang, Zhong-Yi Qin, Junyu Xiang, Dongfeng Chen, Xianfeng Li, Shu-Nan Wang, Chuan Chen, Mengxia Li, Fan Li, Zhenning Wang, Bin Wang","doi":"10.1002/mco2.762","DOIUrl":null,"url":null,"abstract":"<p>Neoadjuvant immunochemotherapy (NAIC) achieves superior clinical benefits over neoadjuvant chemotherapy (NAC) in multiple types of human cancers, including gastric adenocarcinoma (GAC). However, it is poorly understood how the malignant epithelial cells and tumor immune microenvironment (TIME) might respond distinctly to NAIC and NAC that underlies therapeutic efficacy. Here treatment-naive and paired tumor tissues from multiple centers were subjected to pathological, immunological, and transcriptomic analysis. NAIC demonstrated significantly increased rate of pathological complete response compared to NAC (pCR: 25% vs. 4%, <i>p </i>< 0.05). Interestingly, pretreatment intestinal subtype of Lauren's classification was predictive of pathologic regression following NAIC, but not NAC. A substantial portion of cancers underwent intestinal-to-diffuse transition, which occurred less following NAIC and correlated with treatment failure. Moreover, NAIC prevented reprogramming to an immunosuppressive TIME with less active fibroblasts and exhausted CD8<sup>+</sup> T cells, and increased numbers of mature tertiary lymphoid structures. Mechanistically, activation of the tumor necrosis factor alpha (TNFα)/nuclear factor-kappa B (NF-κB) signaling pathway was associated with response to NAIC. Together, NAIC is superior to NAC for locally advanced GAC, likely due to reduced intestinal-to-diffuse conversion and reprogramming to an immuno-active TIME. Modulation of the histological conversion and immunosuppressive TIME could be translatable approaches to improve neoadjuvant therapeutic efficacy.</p>","PeriodicalId":94133,"journal":{"name":"MedComm","volume":null,"pages":null},"PeriodicalIF":10.7000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mco2.762","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MedComm","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mco2.762","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
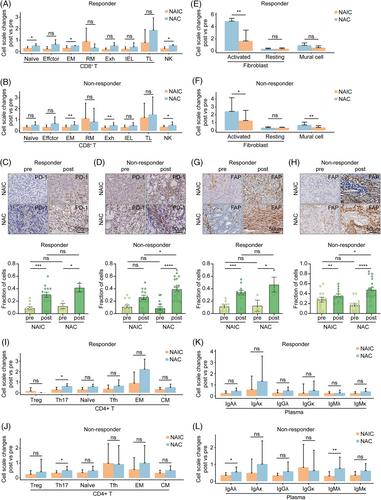
Neoadjuvant immunochemotherapy (NAIC) achieves superior clinical benefits over neoadjuvant chemotherapy (NAC) in multiple types of human cancers, including gastric adenocarcinoma (GAC). However, it is poorly understood how the malignant epithelial cells and tumor immune microenvironment (TIME) might respond distinctly to NAIC and NAC that underlies therapeutic efficacy. Here treatment-naive and paired tumor tissues from multiple centers were subjected to pathological, immunological, and transcriptomic analysis. NAIC demonstrated significantly increased rate of pathological complete response compared to NAC (pCR: 25% vs. 4%, p < 0.05). Interestingly, pretreatment intestinal subtype of Lauren's classification was predictive of pathologic regression following NAIC, but not NAC. A substantial portion of cancers underwent intestinal-to-diffuse transition, which occurred less following NAIC and correlated with treatment failure. Moreover, NAIC prevented reprogramming to an immunosuppressive TIME with less active fibroblasts and exhausted CD8+ T cells, and increased numbers of mature tertiary lymphoid structures. Mechanistically, activation of the tumor necrosis factor alpha (TNFα)/nuclear factor-kappa B (NF-κB) signaling pathway was associated with response to NAIC. Together, NAIC is superior to NAC for locally advanced GAC, likely due to reduced intestinal-to-diffuse conversion and reprogramming to an immuno-active TIME. Modulation of the histological conversion and immunosuppressive TIME could be translatable approaches to improve neoadjuvant therapeutic efficacy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


