Efficacy and safety of endoscopic ultrasonography (EUS) hepaticogastrostomy (HGS) versus choledochoduodenostomy (CDS) in ERCP-failed malignant biliary obstruction: A systematic review and META-analysis
Chrisandi Y Rizqiansyah, Putu I D Awatara, Nasim Amar, Cosmas R A Lesmana, Syifa Mustika
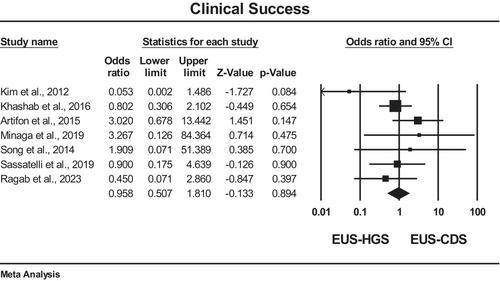
{"title":"Efficacy and safety of endoscopic ultrasonography (EUS) hepaticogastrostomy (HGS) versus choledochoduodenostomy (CDS) in ERCP-failed malignant biliary obstruction: A systematic review and META-analysis","authors":"Chrisandi Y Rizqiansyah, Putu I D Awatara, Nasim Amar, Cosmas R A Lesmana, Syifa Mustika","doi":"10.1002/jgh3.70037","DOIUrl":null,"url":null,"abstract":"<p>Endoscopic retrograde cholangiopancreatography (ERCP) is the gold standard in managing malignant biliary obstruction. The success of ERCP has limitations, whereas surgical biliary bypass and percutaneous transhepatic approaches, as alternative modalities, come with significant costs, longer durations, and higher levels of mortality and morbidity. Endoscopic ultrasonography (EUS)-guided biliary drainage with two approaches, hepaticogastrostomy (EUS-HGS) and choledochoduodenostomy (EUS-CDS), is a favored and evolving alternative modality. This study aims to compare the efficacy and safety of EUS-HGS and EUS-CDS. We conducted a systematic review and meta-analysis by searching PubMed, ScienceDirect, Cochrane Library, and Scholar databases up to August 2023, based on the 2020 PRISMA guidelines. We identified randomized and nonrandomized studies comparing the efficacy and safety of EUS-HGS and EUS-CDS. Outcome measures included technical and clinical success, side effects, and mean procedure time. Nine nonrandomized studies and two randomized controlled trials involving 537 patients (225 EUS-HGS, 312 EUS-CDS) were analyzed. No difference was found in technical success (OR, 0.83; 95% CI, 0.41–1.68; <i>I</i><sup>2</sup> = 0%) and clinical success between the two procedures (OR, 0.96; 95% CI, 0.51–1.81; <i>I</i><sup>2</sup> = 9.94%). Side effects were significantly higher in EUS-HGS (OR, 2.01, 95% CI, 1.14–3.59; <i>I</i><sup>2</sup> = 0%). No significant difference in mean procedure time was observed between the two procedures (0.13; 95% CI, −0.15–0.41; <i>I</i><sup>2</sup> = 34.89%). There are differences in efficacy and safety between EUS-HGS and EUS-CDS. EUS-CDS has a faster procedure time, lower risk of side effects, and ease of puncture during the procedure.</p>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 10","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11494398/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70037","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) is the gold standard in managing malignant biliary obstruction. The success of ERCP has limitations, whereas surgical biliary bypass and percutaneous transhepatic approaches, as alternative modalities, come with significant costs, longer durations, and higher levels of mortality and morbidity. Endoscopic ultrasonography (EUS)-guided biliary drainage with two approaches, hepaticogastrostomy (EUS-HGS) and choledochoduodenostomy (EUS-CDS), is a favored and evolving alternative modality. This study aims to compare the efficacy and safety of EUS-HGS and EUS-CDS. We conducted a systematic review and meta-analysis by searching PubMed, ScienceDirect, Cochrane Library, and Scholar databases up to August 2023, based on the 2020 PRISMA guidelines. We identified randomized and nonrandomized studies comparing the efficacy and safety of EUS-HGS and EUS-CDS. Outcome measures included technical and clinical success, side effects, and mean procedure time. Nine nonrandomized studies and two randomized controlled trials involving 537 patients (225 EUS-HGS, 312 EUS-CDS) were analyzed. No difference was found in technical success (OR, 0.83; 95% CI, 0.41–1.68; I2 = 0%) and clinical success between the two procedures (OR, 0.96; 95% CI, 0.51–1.81; I2 = 9.94%). Side effects were significantly higher in EUS-HGS (OR, 2.01, 95% CI, 1.14–3.59; I2 = 0%). No significant difference in mean procedure time was observed between the two procedures (0.13; 95% CI, −0.15–0.41; I2 = 34.89%). There are differences in efficacy and safety between EUS-HGS and EUS-CDS. EUS-CDS has a faster procedure time, lower risk of side effects, and ease of puncture during the procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


