Surgical resection and overall survival in cT4b sinonasal non-squamous cell carcinoma
Abstract
Objective
Surgical resection is associated with higher overall survival (OS) than definitive radiotherapy (RT) or chemoradiotherapy (CRT) in cT4b sinonasal squamous cell carcinoma (SCC). Our study investigates the survival benefit of surgical resection in cT4b sinonasal non-SCC.
Methods
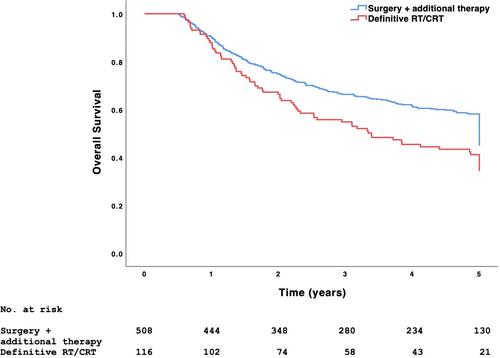
The 2004 to 2019 National Cancer Database was queried for patients with cT4b sinonasal non-SCC undergoing definitive treatment with (1) surgical resection + additional therapy (RT, chemotherapy, or both), (2) RT alone, or (3) CRT. Surgical resection + additional therapy and definitive RT/CRT were compared with Kaplan–Meier and multivariable Cox regression models.
Results
Of 629 patients satisfying inclusion criteria, 513 (81.6%) underwent surgical resection + additional therapy and 116 (18.4%) underwent definitive RT/CRT. The most frequent histologic types were undifferentiated carcinoma (23.7%), adenoid cystic carcinoma (22.6%), and adenocarcinoma (20.7%). Few patients presented with clinical nodal metastasis (15.7%). There were 4 (0.8%) mortalities within 90 days of surgical resection. Patients undergoing surgical resection with positive surgical margins had higher 5-year OS than those undergoing definitive RT/CRT (56.3% vs. 39.4%, p = .039) and similar 5-year OS as those with negative margins (56.3% vs. 63.9%, p = .059). Patients undergoing neoadjuvant chemotherapy had similar 5-year OS as those undergoing definitive RT/CRT (60.9% vs. 39.5%, p = .053). Age at diagnosis, tumor diameter, and surgical resection + additional therapy (aHR 0.64, 95% CI 0.45–0.91) were associated with OS (p < .05).
Conclusion
Surgical resection + additional therapy was associated with higher OS than definitive RT/CRT in cT4b sinonasal non-SCC. Surgical resection may benefit select patient with cT4b sinonasal non-SCC.
Level of Evidence
4.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


