Catriona Matheson, Chris Vucic, Josh Dumbrell, Roy Robertson, Trina Ritchie, Clare Duncan, Karthigayan Kessavalou, Caroline Woolston, Joe Schofield
{"title":"Clinical Outcomes of Benzodiazepine Prescribing for People Receiving Opioid Agonist Treatment: A Systematic Review of the Evidence.","authors":"Catriona Matheson, Chris Vucic, Josh Dumbrell, Roy Robertson, Trina Ritchie, Clare Duncan, Karthigayan Kessavalou, Caroline Woolston, Joe Schofield","doi":"10.3390/pharmacy12050152","DOIUrl":null,"url":null,"abstract":"<p><p>Many countries are experiencing an increased use of unregulated benzodiazepines in combination with opioids and other drugs, which contributes to drug-related harm. This descriptive review identifies and synthesises the outcomes of studies co-prescribing benzodiazepines and opioids. A systematic review was undertaken in Medline, CINAHL, PsychInfo, Embase, and the Cochrane databases covering publications from 1 January 1991 to 18 November 2021. Inclusion criteria were peer reviewed, English language studies of adults prescribed opioid agonist treatment (OAT) and a concurrent benzodiazepine, and reporting outcome data. Of the 4370 titles screened, 18 papers were included. The main outcomes identified covered all-cause mortality (ACM) (n = 5); overdose death (n = 3); retention in treatment (n = 7); and hospitalisation/emergency department encounters (n = 2). Other outcomes included QTc interval, cognitive function, illicit drug use, and mental health. The prescription of benzodiazepines alongside OAT increased the ACM by 75-90%, while evidence on overdose death was less robust but indicative of increased risk (40-334%). There was an indicative positive effect on treatment retention, with increased retention in those prescribed a benzodiazepine with OAT compared to those not prescribed or taking non-prescribed benzodiazepines. In conclusion, methodologically robust epidemiological studies found increased ACM and overdose death but possibly improved retention. However confounders (e.g., psychiatric comorbidity) exist, so a trial is recommended.</p>","PeriodicalId":30544,"journal":{"name":"Pharmacy","volume":"12 5","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511121/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pharmacy12050152","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
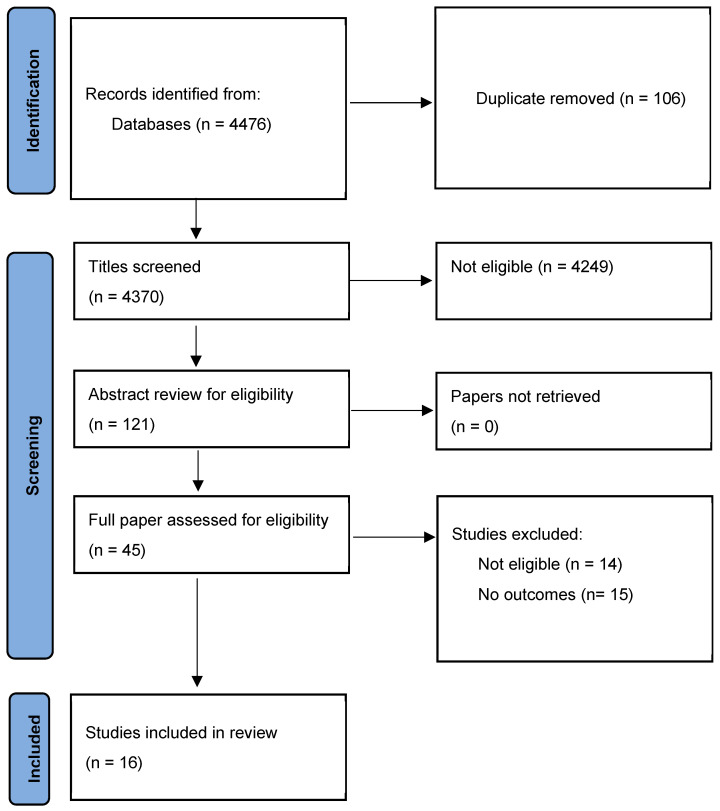
Many countries are experiencing an increased use of unregulated benzodiazepines in combination with opioids and other drugs, which contributes to drug-related harm. This descriptive review identifies and synthesises the outcomes of studies co-prescribing benzodiazepines and opioids. A systematic review was undertaken in Medline, CINAHL, PsychInfo, Embase, and the Cochrane databases covering publications from 1 January 1991 to 18 November 2021. Inclusion criteria were peer reviewed, English language studies of adults prescribed opioid agonist treatment (OAT) and a concurrent benzodiazepine, and reporting outcome data. Of the 4370 titles screened, 18 papers were included. The main outcomes identified covered all-cause mortality (ACM) (n = 5); overdose death (n = 3); retention in treatment (n = 7); and hospitalisation/emergency department encounters (n = 2). Other outcomes included QTc interval, cognitive function, illicit drug use, and mental health. The prescription of benzodiazepines alongside OAT increased the ACM by 75-90%, while evidence on overdose death was less robust but indicative of increased risk (40-334%). There was an indicative positive effect on treatment retention, with increased retention in those prescribed a benzodiazepine with OAT compared to those not prescribed or taking non-prescribed benzodiazepines. In conclusion, methodologically robust epidemiological studies found increased ACM and overdose death but possibly improved retention. However confounders (e.g., psychiatric comorbidity) exist, so a trial is recommended.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


