Clinical and Cost-Effectiveness of Intraoperative Flap Perfusion Assessment With Indocyanine Green Fluorescence Angiography in Breast and Head and Neck Reconstructions: A Systematic Review and Meta-Analysis
Abstract
Background
Indocyanine green fluorescence angiography (ICGFA) is gaining popularity for the assessment of reconstructive flap perfusion intraoperatively. This study analyses the literature with a focus on its clinical efficacy and cost-effectiveness across various plastic and reconstructive surgery procedures.
Methods
A systematic review was conducted in accordance with PRISMA guidelines on published studies in English comparing ICGFA with standard clinical assessment for flap perfusion. Meta-analysis concerned perfusion-related complications and cost data.
Results
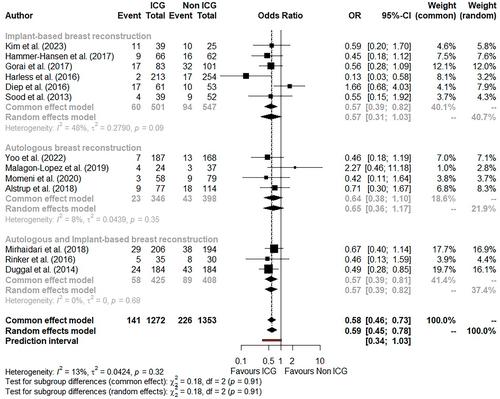
Twenty-five studies met the inclusion criteria, of which two were randomized controlled trials (RCTs) and four were prospective cohort studies. Twenty-one studies were AHRQ Standard ‘Good’; however, the overall level of evidence remains low. ICGFA was predominantly performed in breast surgeries (n = 3310) and head and neck reconstruction (n = 701) albeit with inconsistency in protocols and predominantly subjective interpretations (only five studies utilized objective thresholds). In breast surgery, meta-analysis demonstrated significant reductions in mastectomy skin flap necrosis (odds ratio (OR) 0.58, p < 0.0001), fat necrosis (OR 0.31, p < 0.001), infection (OR 0.66, p = 0.02), and re-operation (OR 0.40, p < 0.0001), but no significant decrease in total or partial flap loss (OR 0.78, p = 0.57/OR 0.87, p = 0.56, respectively) or increase in dehiscence (OR 1.55, p = 0.11). In head and neck surgery, ICGFA significantly decreased total flap loss (OR 0.47, p = 0.04), although not partial flap loss (OR 0.37, p = 0.13) and reoperation (OR 0.92, p = 0.73). Lower limb (n = 104) and abdominal wall (n = 95) reconstructive surgeries were much less studied with no significant ICGFA impact. Seven studies reported cost savings with flap surgeries and breast reconstructions, although study heterogeneity precluded meta-analysis.
Conclusions
ICGFA appears to be a useful, cost-effective tool to identify otherwise unsuspected hypoperfusion in breast and head and neck reconstruction. There is a clear need for standardization, however, to avoid bias. Further RCTs are necessary to solidify these promising clinical findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


