{"title":"Fears for tears? Targeted therapies for atopic dermatitis and ocular surface health","authors":"Carolyn Jack, Aaron M. Drucker","doi":"10.1111/jdv.20356","DOIUrl":null,"url":null,"abstract":"<p>Dupilumab is a monoclonal antibody that binds the IL-4 receptor alpha to block a key cytokine axis in atopy, with an excellent safety profile from infancy through old age. In a minority of patients with atopic dermatitis (AD), Dupilumab can be associated with worsening or new inflammation at the surface of the eye.<span><sup>1</sup></span> For most patients, this adverse event is mild or readily managed; but for some, it can lead to Dupilumab discontinuation. Reguiai et al.<span><sup>1</sup></span> have sought to describe this population with a 12-site French collaborative study and contribute new real-world information that may help to address ongoing gaps in knowledge at this ocular epithelial frontier.</p><p>The ocular surface is a dynamic mucosal system that provides lubrication to the eye as well as physical and immunological defence, see Figure 1a. Common criteria for AD include five features involving the eyes: conjunctivitis, keratoconus, cataracts and two signs of peri-orbital skin changes. Conjunctivitis is prevalent in nearly one third of AD patients, and there may be a causal effect from the skin to the eyes.<span><sup>2</sup></span> Shi et al.<span><sup>3</sup></span> recently provided an excellent overview of ocular surface disease (OSD), comprehensive of pathobiology and clinical outcomes in AD patients. More than half of adult AD patients eligible for systemic therapies may suffer from eye symptoms such as pruritus, and a majority can show signs of blepharitis and conjunctivitis, where the hidden palpebral conjunctiva is more commonly affected than that covering the orbit.<span><sup>4</sup></span> These findings may account for the higher rates of ocular adverse effects in pivotal Dupilumab studies for AD, versus asthma or nasal polyposis.<span><sup>3</sup></span></p><p>The Reguiai cohort included 83 patients (7.5% of 1109 Dupilumab-treated patients) who developed OSD leading to treatment switch; 71 patients were captured in follow-up, and 73% were assessed by ophthalmology (Figure 1b).<span><sup>1</sup></span> Most cases were mild–moderate forms of blepharo-conjunctivitis, the subtype of OSD most strongly associated with AD.<span><sup>1, 3</sup></span> Sixty-five % of patients were initially switched to a JAK inhibitor (JAKi) and 35% to the anti-IL-13 biologic Tralokinumab.<span><sup>1</sup></span> Although 30% of patients were subsequently switched again, 68% remained on a JAKi and 7% restarted Dupilumab.<span><sup>1</sup></span> At the end of the study, nearly one quarter of OSD patients had persistent disease, with slightly more still using topical therapies.<span><sup>1</sup></span> While the sample size of the cohort is small, leading to wide confidence intervals for the regression analyses, they did find significantly increased odds for complete resolution associated with switching to a JAKi.<span><sup>1</sup></span>.</p><p>Recent studies have helped initiate a mechanistic framework for understanding Dupilumab-associated OSD (DAOSD), which appears to involve increased Th1-type inflammatory pathways, remodelling mediators and stable goblet cell numbers yet lower mucin production.<span><sup>4, 5</sup></span> DAOSD may differ from allergic-type or AD-associated pathology characterized by increased and decreased goblet cells, respectively, although current data is quite limited.<span><sup>4</sup></span> As 44% of patients in the Reguiai cohort reported a history of conjunctivitis at baseline, and as patients with DAOSD who did not switch therapy are not included in this cohort, the factors contributing to a high prevalence of persistent OSD among all those who develop it remain unclear.<span><sup>1</sup></span></p><p>When considering atopic disease through the lens of systemic immune dysfunction, we can now coordinate the control of inflammation at most epithelial surfaces using systemic therapies. There remains a gap in understanding refractory, paradoxical and organ-specific pathways of immune dysfunction, including ocular surface inflammation with Dupilumab, as well as with skin- or airway-specific responses to IL-13 and IL-5 blockade, respectively. While focused on adults, the results of this study are an important reminder to Dermatologists to consider ocular health in their AD patients, particularly those considering systemic therapy, and add increasing weight to the rationale that patient outcomes may be improved by considering this multi-epithelial disorder holistically.</p><p>C. Jack reports grants from the Montreal Dermatology Research Institute, Fonds de Recherche du Québec - Santé (FRQS), SkIN Canada, Programme d’aide à l’entrepreneuriat (PAEN), Mackenzie I. Watson Educational Grant, Innovaderm Research, McGill University Department of Medicine, McGill CPD MedUpdates, MITACS, Canadian Dermatology Foundation, Canadian Dermatology Association, and Eczema Society of Canada, as well as grants, involvement in clinical studies, and/or consultancy work for Sanofi, Eli Lilly, AbbVie, Novartis, Valeant, Bausch, Pfizer, Amgen, Celgene, Janssen, Boehringer Ingelheim, Asana, LEO, Dermavant, AntibioTx, Neokera, Kiniksa, Ralexar, Arcutis, BMS, Boston, Cara, Concert, Incyte, Sienna, Aristea, Target PharmaSolution, Lyceum Health, LaRoche-Posay, Johnson & Johnson Inc., L'Oreal, Chronicle, Catalytic, Beiersdorf, Innomar, Apogee Therapeutics, Galderma, LEAD, and UCB. Dr. Drucker has received compensation from the British Journal of Dermatology (reviewer and Section Editor), American Academy of Dermatology (guidelines writer), Canadian Dermatology Today (manuscript writer), and National Eczema Association (consultant) Canadian Agency for Drugs and Technologies in Health (consultant). Dr. Drucker has received research grants to his institution from the National Eczema Association, Eczema Society of Canada, Canadian Dermatology Foundation, Canadian Institutes for Health Research, US National Institutes of Health and Physicians Services Incorporated Foundation.</p>","PeriodicalId":17351,"journal":{"name":"Journal of the European Academy of Dermatology and Venereology","volume":"38 11","pages":"2053-2055"},"PeriodicalIF":8.4000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdv.20356","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the European Academy of Dermatology and Venereology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jdv.20356","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Dupilumab is a monoclonal antibody that binds the IL-4 receptor alpha to block a key cytokine axis in atopy, with an excellent safety profile from infancy through old age. In a minority of patients with atopic dermatitis (AD), Dupilumab can be associated with worsening or new inflammation at the surface of the eye.1 For most patients, this adverse event is mild or readily managed; but for some, it can lead to Dupilumab discontinuation. Reguiai et al.1 have sought to describe this population with a 12-site French collaborative study and contribute new real-world information that may help to address ongoing gaps in knowledge at this ocular epithelial frontier.
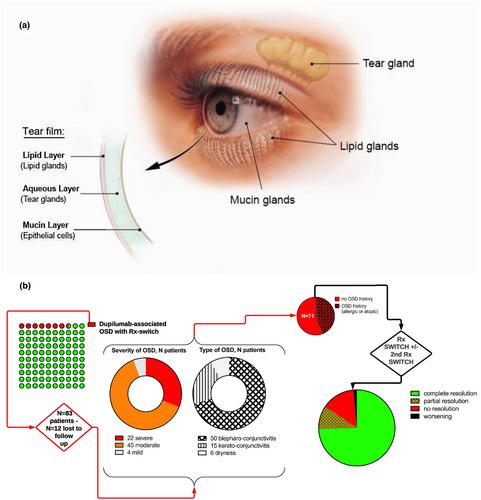
The ocular surface is a dynamic mucosal system that provides lubrication to the eye as well as physical and immunological defence, see Figure 1a. Common criteria for AD include five features involving the eyes: conjunctivitis, keratoconus, cataracts and two signs of peri-orbital skin changes. Conjunctivitis is prevalent in nearly one third of AD patients, and there may be a causal effect from the skin to the eyes.2 Shi et al.3 recently provided an excellent overview of ocular surface disease (OSD), comprehensive of pathobiology and clinical outcomes in AD patients. More than half of adult AD patients eligible for systemic therapies may suffer from eye symptoms such as pruritus, and a majority can show signs of blepharitis and conjunctivitis, where the hidden palpebral conjunctiva is more commonly affected than that covering the orbit.4 These findings may account for the higher rates of ocular adverse effects in pivotal Dupilumab studies for AD, versus asthma or nasal polyposis.3
The Reguiai cohort included 83 patients (7.5% of 1109 Dupilumab-treated patients) who developed OSD leading to treatment switch; 71 patients were captured in follow-up, and 73% were assessed by ophthalmology (Figure 1b).1 Most cases were mild–moderate forms of blepharo-conjunctivitis, the subtype of OSD most strongly associated with AD.1, 3 Sixty-five % of patients were initially switched to a JAK inhibitor (JAKi) and 35% to the anti-IL-13 biologic Tralokinumab.1 Although 30% of patients were subsequently switched again, 68% remained on a JAKi and 7% restarted Dupilumab.1 At the end of the study, nearly one quarter of OSD patients had persistent disease, with slightly more still using topical therapies.1 While the sample size of the cohort is small, leading to wide confidence intervals for the regression analyses, they did find significantly increased odds for complete resolution associated with switching to a JAKi.1.
Recent studies have helped initiate a mechanistic framework for understanding Dupilumab-associated OSD (DAOSD), which appears to involve increased Th1-type inflammatory pathways, remodelling mediators and stable goblet cell numbers yet lower mucin production.4, 5 DAOSD may differ from allergic-type or AD-associated pathology characterized by increased and decreased goblet cells, respectively, although current data is quite limited.4 As 44% of patients in the Reguiai cohort reported a history of conjunctivitis at baseline, and as patients with DAOSD who did not switch therapy are not included in this cohort, the factors contributing to a high prevalence of persistent OSD among all those who develop it remain unclear.1
When considering atopic disease through the lens of systemic immune dysfunction, we can now coordinate the control of inflammation at most epithelial surfaces using systemic therapies. There remains a gap in understanding refractory, paradoxical and organ-specific pathways of immune dysfunction, including ocular surface inflammation with Dupilumab, as well as with skin- or airway-specific responses to IL-13 and IL-5 blockade, respectively. While focused on adults, the results of this study are an important reminder to Dermatologists to consider ocular health in their AD patients, particularly those considering systemic therapy, and add increasing weight to the rationale that patient outcomes may be improved by considering this multi-epithelial disorder holistically.
C. Jack reports grants from the Montreal Dermatology Research Institute, Fonds de Recherche du Québec - Santé (FRQS), SkIN Canada, Programme d’aide à l’entrepreneuriat (PAEN), Mackenzie I. Watson Educational Grant, Innovaderm Research, McGill University Department of Medicine, McGill CPD MedUpdates, MITACS, Canadian Dermatology Foundation, Canadian Dermatology Association, and Eczema Society of Canada, as well as grants, involvement in clinical studies, and/or consultancy work for Sanofi, Eli Lilly, AbbVie, Novartis, Valeant, Bausch, Pfizer, Amgen, Celgene, Janssen, Boehringer Ingelheim, Asana, LEO, Dermavant, AntibioTx, Neokera, Kiniksa, Ralexar, Arcutis, BMS, Boston, Cara, Concert, Incyte, Sienna, Aristea, Target PharmaSolution, Lyceum Health, LaRoche-Posay, Johnson & Johnson Inc., L'Oreal, Chronicle, Catalytic, Beiersdorf, Innomar, Apogee Therapeutics, Galderma, LEAD, and UCB. Dr. Drucker has received compensation from the British Journal of Dermatology (reviewer and Section Editor), American Academy of Dermatology (guidelines writer), Canadian Dermatology Today (manuscript writer), and National Eczema Association (consultant) Canadian Agency for Drugs and Technologies in Health (consultant). Dr. Drucker has received research grants to his institution from the National Eczema Association, Eczema Society of Canada, Canadian Dermatology Foundation, Canadian Institutes for Health Research, US National Institutes of Health and Physicians Services Incorporated Foundation.
期刊介绍:
The Journal of the European Academy of Dermatology and Venereology (JEADV) is a publication that focuses on dermatology and venereology. It covers various topics within these fields, including both clinical and basic science subjects. The journal publishes articles in different formats, such as editorials, review articles, practice articles, original papers, short reports, letters to the editor, features, and announcements from the European Academy of Dermatology and Venereology (EADV).
The journal covers a wide range of keywords, including allergy, cancer, clinical medicine, cytokines, dermatology, drug reactions, hair disease, laser therapy, nail disease, oncology, skin cancer, skin disease, therapeutics, tumors, virus infections, and venereology.
The JEADV is indexed and abstracted by various databases and resources, including Abstracts on Hygiene & Communicable Diseases, Academic Search, AgBiotech News & Information, Botanical Pesticides, CAB Abstracts®, Embase, Global Health, InfoTrac, Ingenta Select, MEDLINE/PubMed, Science Citation Index Expanded, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


