{"title":"Acute Allograft Rejection in Kidney Transplant Recipients Treated With Immune Checkpoint Inhibitors: An Educational Case Report.","authors":"Steven A Morrison, Amanda J Vinson","doi":"10.1177/20543581241289191","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>Kidney transplant (KT) recipients have an increased risk of malignancy due to chronic immunosuppression. The emerging use of immune checkpoint inhibitors (ICIs) has been a promising development for the treatment of malignancy, but their use adds to the complexity of immunosuppression management for KT recipients. This case report describes 2 cases of acute rejection in KT recipients following ICI initiation and discusses the balance of malignancy treatment with adequate immunosuppression.</p><p><strong>Presenting concerns of patients: </strong>The first patient is a 44-year-old male KT recipient with a diagnosis of metastatic renal cell carcinoma presenting with acute kidney injury 6 days following initiation of an ICI. The second patient is a 73-year-old male KT recipient with a diagnosis of squamous cell carcinoma presenting with acute kidney injury 2 weeks following initiation of an ICI.</p><p><strong>Diagnoses: </strong>Both patients were diagnosed with acute rejection in the setting of reduced immunosuppression and initiation of an ICI.</p><p><strong>Interventions: </strong>Both cases received an increased dose of steroid without improvement of graft function. The first patient subsequently underwent a delayed graft nephrectomy due to complications of acute rejection, whereas the second patient did not undergo nephrectomy.</p><p><strong>Outcomes: </strong>The first patient experienced complications including perioperative bleeding requiring multiple operations, but ultimately stabilized on hemodialysis and showed a durable response to ICI. The second patient remained dialysis-dependent post-ICI treatment and was readmitted with allograft complications leading to his eventual death.</p><p><strong>Teaching points: </strong>This study underscores the complexity of managing KT recipients diagnosed with malignancy and receiving ICIs. The balance between immunosuppression reduction to treat malignancy and preventing allograft rejection presents a significant challenge. Key considerations include the risk of acute allograft rejection and patient-centered decision-making. These cases highlight the need for further research to develop evidence-based guidelines for managing this patient population. In addition, the patient perspective in this study highlights the importance of careful risk-benefit analysis and the impact of treatment decisions on patient-focused outcomes.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241289191"},"PeriodicalIF":1.5000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11497508/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241289191","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Rationale: Kidney transplant (KT) recipients have an increased risk of malignancy due to chronic immunosuppression. The emerging use of immune checkpoint inhibitors (ICIs) has been a promising development for the treatment of malignancy, but their use adds to the complexity of immunosuppression management for KT recipients. This case report describes 2 cases of acute rejection in KT recipients following ICI initiation and discusses the balance of malignancy treatment with adequate immunosuppression.
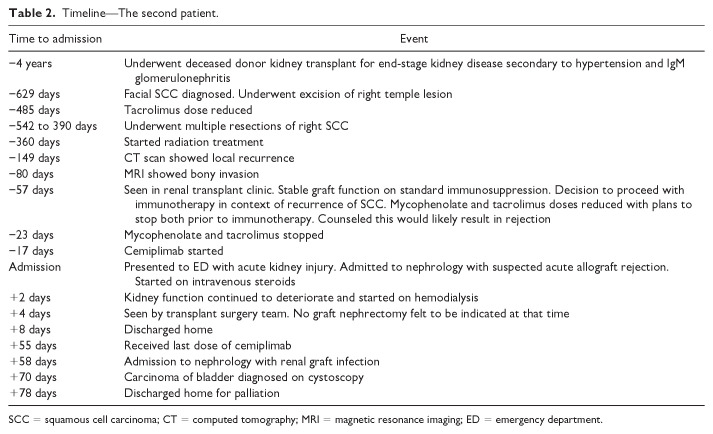
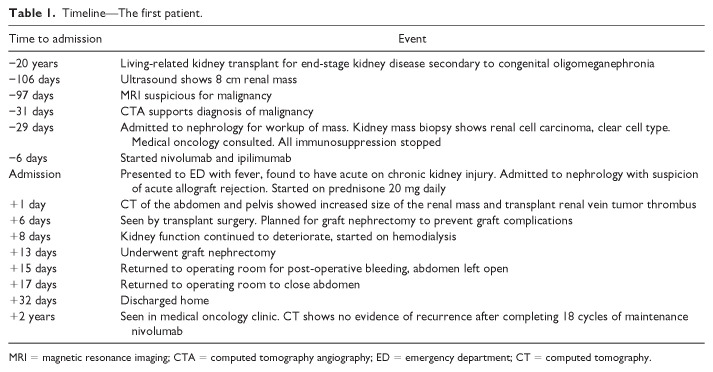
Presenting concerns of patients: The first patient is a 44-year-old male KT recipient with a diagnosis of metastatic renal cell carcinoma presenting with acute kidney injury 6 days following initiation of an ICI. The second patient is a 73-year-old male KT recipient with a diagnosis of squamous cell carcinoma presenting with acute kidney injury 2 weeks following initiation of an ICI.
Diagnoses: Both patients were diagnosed with acute rejection in the setting of reduced immunosuppression and initiation of an ICI.
Interventions: Both cases received an increased dose of steroid without improvement of graft function. The first patient subsequently underwent a delayed graft nephrectomy due to complications of acute rejection, whereas the second patient did not undergo nephrectomy.
Outcomes: The first patient experienced complications including perioperative bleeding requiring multiple operations, but ultimately stabilized on hemodialysis and showed a durable response to ICI. The second patient remained dialysis-dependent post-ICI treatment and was readmitted with allograft complications leading to his eventual death.
Teaching points: This study underscores the complexity of managing KT recipients diagnosed with malignancy and receiving ICIs. The balance between immunosuppression reduction to treat malignancy and preventing allograft rejection presents a significant challenge. Key considerations include the risk of acute allograft rejection and patient-centered decision-making. These cases highlight the need for further research to develop evidence-based guidelines for managing this patient population. In addition, the patient perspective in this study highlights the importance of careful risk-benefit analysis and the impact of treatment decisions on patient-focused outcomes.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


