Statin use is associated with less ST-elevation versus non-ST-elevation myocardial infarction in a nationwide study
IF 4.9
2区 医学
Q1 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background and aims
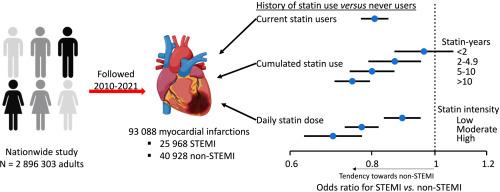
Statin therapy reduces myocardial infarction rate but whether it is associated with a shift of ST-elevation myocardial infarction (STEMI) towards non-ST-elevation myocardial infarction (non-STEMI) remains unknown. Thus, we tested the hypothesis that statin use is associated with less STEMI relative to non-STEMI in first-time myocardial infarction.
Methods
In a nationwide study, including 66,896 patients with first-time myocardial infarction between 2010 and 2021, we obtained multivariable risk estimates for STEMI versus non-STEMI according to any statin use, cumulated statin use, and daily statin dose. Furthermore, we obtained hazard ratios for 60-day mortality (5545 deaths) following myocardial infarction according to type of infarction.
Results
Odds ratios for STEMI versus non-STEMI were 0.81 (95 % CI:0.77–0.85) and 1.07 (1.01–1.13) in current and previous statin users compared to never statin users. Cumulated statin exposure yielded odds ratios of 0.96 (0.87–1.07) for <2 statin-years, 0.87 (0.79–0.95) for 2–4.9 statin-years, 0.80 (0.74–0.87) for 5–10 statin-years, and 0.75 (0.70–0.80) for >10 statin-years compared to never users. Corresponding odds ratios for statin dose intensity were 0.89 (0.84–0.95) for low-intensity, 0.77 (0.73–0.82) for moderate-intensity, and 0.70 (0.63–0.77) for high-intensity. Results were similar in multiple sensitivity analyses and using a cohort design. The hazard ratio for 60-day mortality after first-time STEMI versus non-STEMI was 2.24 (2.13–2.37).
Conclusions
In this nationwide study, prior statin use is associated with less STEMI relative to non-STEMI in a dose dependent manner. This indicates that statin therapy, in addition to reducing myocardial infarction event rates, also result in a less severe presentation of myocardial infarctions.
在一项全国性研究中,使用他汀类药物可减少ST段抬高与非ST段抬高心肌梗死的发生率。
背景和目的:他汀类药物治疗可降低心肌梗死发生率,但它是否与ST段抬高型心肌梗死(STEMI)向非ST段抬高型心肌梗死(非STEMI)的转变有关仍是未知数。因此,我们对他汀类药物的使用与首次心肌梗死中STEMI相对于非STEMI的减少有关这一假设进行了检验:在一项全国性研究(包括 2010 年至 2021 年间的 66,896 例首次心肌梗死患者)中,我们根据是否使用过他汀类药物、累计使用他汀类药物的情况以及他汀类药物的日剂量,得出了 STEMI 与非 STEMI 的多变量风险估计值。此外,我们还根据心肌梗死类型得出了心肌梗死后 60 天死亡率(5545 例死亡)的危险比:与从未使用过他汀类药物的患者相比,目前和曾经使用过他汀类药物的患者STEMI与非STEMI的危险比分别为0.81(95 % CI:0.77-0.85)和1.07(1.01-1.13)。与从未使用过他汀类药物者相比,累积他汀类药物暴露 10 年的几率比为 0.96(0.87-1.07)。他汀类药物剂量强度的相应几率比分别为:低强度 0.89(0.84-0.95),中强度 0.77(0.73-0.82),高强度 0.70(0.63-0.77)。多重敏感性分析和队列设计的结果相似。首次 STEMI 后 60 天死亡率与非 STEMI 后 60 天死亡率的危险比为 2.24(2.13-2.37):在这项全国性研究中,他汀类药物的使用剂量与STEMI的发生率相关,而非STEMI的发生率较低。这表明他汀类药物治疗除了能降低心肌梗死的发生率外,还能减少心肌梗死的严重程度。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Atherosclerosis
医学-外周血管病
CiteScore
9.80
自引率
3.80%
发文量
1269
审稿时长
36 days
期刊介绍:
Atherosclerosis has an open access mirror journal Atherosclerosis: X, sharing the same aims and scope, editorial team, submission system and rigorous peer review.
Atherosclerosis brings together, from all sources, papers concerned with investigation on atherosclerosis, its risk factors and clinical manifestations. Atherosclerosis covers basic and translational, clinical and population research approaches to arterial and vascular biology and disease, as well as their risk factors including: disturbances of lipid and lipoprotein metabolism, diabetes and hypertension, thrombosis, and inflammation. The Editors are interested in original or review papers dealing with the pathogenesis, environmental, genetic and epigenetic basis, diagnosis or treatment of atherosclerosis and related diseases as well as their risk factors.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


