Reassess Hospital Costs and Mortality Between Myocardial Infarction With and Without ST-Segment Elevation in a Modern Context
Abstract
Background
Patients with ST-segment elevation myocardial infarction (STEMI) may have higher hospitalization costs and poorer prognosis than non-ST-segment elevation myocardial infarction (NSTEMI).
Methods
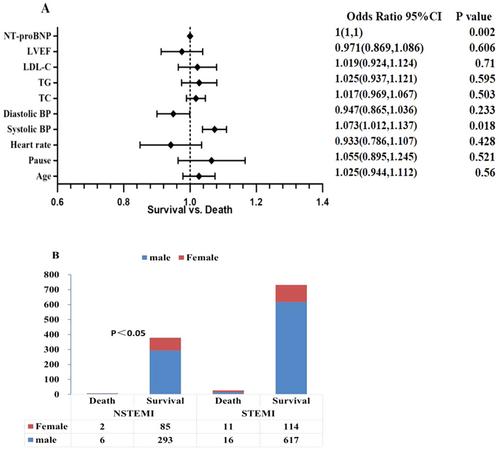
A single-center retrospective study was conducted on 758 STEMI patients and 386 NSTEMI patients from January 1, 2020 to May 30, 2023 aimed to investigate the differences in cost and mortality.
Results
STEMI patients had higher maximal troponin I (15,222.5 (27.18, 40,000.00) vs. 2731.5 (10.73, 27,857.25), p < 0.001) and lower left ventricular ejection fraction (LVEF) (56% (53%, 59%) vs. 57% (55%, 59%), p < 0.001) compared to NSTEMI patients. The clinical symptoms were mainly persistent or interrupted chest pain/distress in either STEMI or NSTEMI patients. STEMI patients had a significantly higher risk of combined hypotension than NSTEMI patients (8.97% vs. 3.89%, p = 0.002), and IABP was much more frequently used in the STEMI group with a statistical difference (2.90% vs. 0.52%, p = 0.015). STEMI patients have statistically higher hospitalization costs (RMB, ¥) (31,667 (25,337.79, 39,790) vs. 30,506.91 (21,405.96, 40,233.75), p = 0.006) and longer hospitalization days (10 (8, 11) vs. 9 (8, 11), p = 0.001) compared to NSTEMI patients. Although in-hospital mortality was higher in STEMI patients, the difference was not statistically significant (3.56% vs. 2.07%, p = 0.167). Multivariable logistic regression was performed and found that systolic blood pressure and NT-proBNP were risk factors for patient death (OR ≥ 1).
Conclusion
STEMI patients are more likely comorbid cardiogenic shock, heart failure complications with higher hospitalization costs and longer hospitalization days. And relatively more use of acute mechanical circulatory support devices such as IABP.
Trial Registration
ChiCTR2300077885

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


