Anticoagulation in the management of septic cavernous sinus thrombosis secondary to rhino-orbito-cerebral mucormycosis: A retrospective real-world experience.
{"title":"Anticoagulation in the management of septic cavernous sinus thrombosis secondary to rhino-orbito-cerebral mucormycosis: A retrospective real-world experience.","authors":"Kiana Amani, Mojtaba Shahbazi, Atefeh Behkar, Ghasem Farahmand, Shima Ghafouri, Sanaz Heydari, Maryam Kaeedi, Hana Magrouni, Fatemeh Alizadeh, Mojdeh Ghabaee, Payam Sarraf, Abbas Tafakhori, Hamed Amirifard, Sakineh Ranji-Burachaloo, Seyed Ehsan Mohammadianinejad, Melika Jameie, Mohammad Hossein Harirchian","doi":"10.18502/cjn.v23i1.16432","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> COVID-19 was associated with an increased number of patients with mucormycosis (MCR), followed by septic cavernous sinus thrombosis (SCST). We evaluated the association between anticoagulation (AC) and mortality/morbidity of COVID-19-associated MCR (CAM)-induced SCST. <b>Methods:</b> In this retrospective study, neurological sequelae, functional outcomes, and in-hospital mortality were compared between AC receivers and non-receivers. In addition, the association between AC and survivability was examined. <b>Results:</b> Twenty-nine patients (17 male; mean age: 51.27 years) with CAM-induced SCST were included in the study. The median intervals between COVID-19 and MCR, and COVID-19 and SCST were 19 and 27 days, respectively. Among AC recipients, the interval between SCST and AC initiation was 18 days, with an AC duration of 37 days. Baseline and management-related characteristics were comparable between AC recipients and non-recipients (P > 0.050). AC receivers (n = 15) and non-receivers (n = 14) did not significantly differ in terms of the proportion of sequelae (6/15 vs. 5/14; P = 1.000), complete recovery (2/15 vs. 4/14; P = 0.687), and in-hospital mortality (3/15 vs. 3/14; P > 0.999). Nevertheless, AC recipients had a longer hospital stay (72.0 vs. 35.5; P = 0.016). AC-related characteristics (AC receiving, type, early initiation, and duration) were not significantly different between survivors and non-survivors, or between recovered and disabled patients. <b>Conclusion:</b> In our study, CAM-induced SCST in-hospital mortality/morbidity did not differ between AC receivers and non-receivers. AC characteristics were not different between survivors and non-survivors, or recovered and disabled patients. However, the small sample size may have limited the ability to detect significant differences, leading to inconclusive results.</p>","PeriodicalId":40077,"journal":{"name":"Current Journal of Neurology","volume":"23 1","pages":"44-58"},"PeriodicalIF":0.5000,"publicationDate":"2024-01-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11489632/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Journal of Neurology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/cjn.v23i1.16432","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
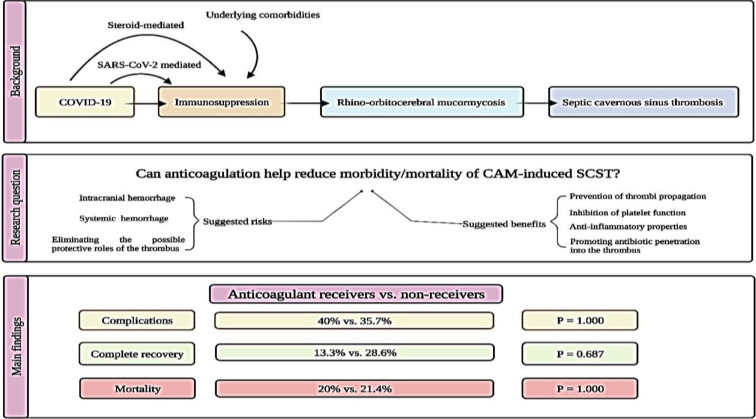
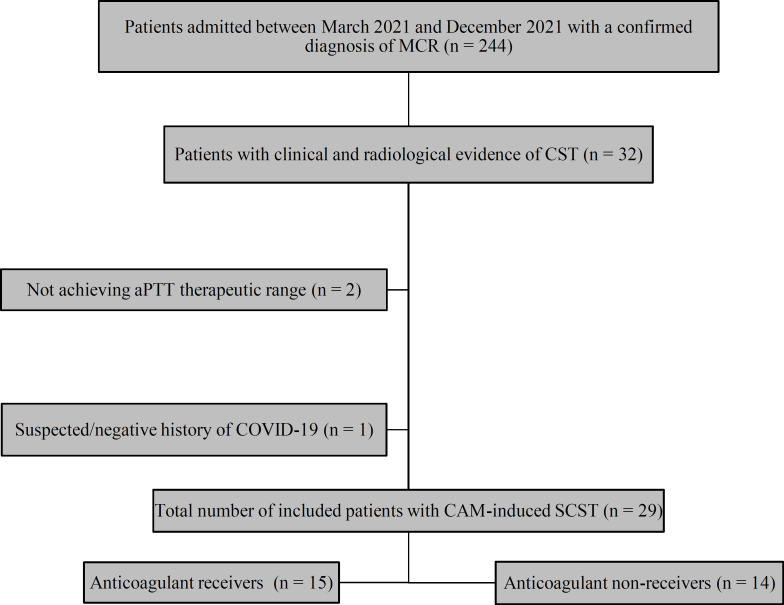
Background: COVID-19 was associated with an increased number of patients with mucormycosis (MCR), followed by septic cavernous sinus thrombosis (SCST). We evaluated the association between anticoagulation (AC) and mortality/morbidity of COVID-19-associated MCR (CAM)-induced SCST. Methods: In this retrospective study, neurological sequelae, functional outcomes, and in-hospital mortality were compared between AC receivers and non-receivers. In addition, the association between AC and survivability was examined. Results: Twenty-nine patients (17 male; mean age: 51.27 years) with CAM-induced SCST were included in the study. The median intervals between COVID-19 and MCR, and COVID-19 and SCST were 19 and 27 days, respectively. Among AC recipients, the interval between SCST and AC initiation was 18 days, with an AC duration of 37 days. Baseline and management-related characteristics were comparable between AC recipients and non-recipients (P > 0.050). AC receivers (n = 15) and non-receivers (n = 14) did not significantly differ in terms of the proportion of sequelae (6/15 vs. 5/14; P = 1.000), complete recovery (2/15 vs. 4/14; P = 0.687), and in-hospital mortality (3/15 vs. 3/14; P > 0.999). Nevertheless, AC recipients had a longer hospital stay (72.0 vs. 35.5; P = 0.016). AC-related characteristics (AC receiving, type, early initiation, and duration) were not significantly different between survivors and non-survivors, or between recovered and disabled patients. Conclusion: In our study, CAM-induced SCST in-hospital mortality/morbidity did not differ between AC receivers and non-receivers. AC characteristics were not different between survivors and non-survivors, or recovered and disabled patients. However, the small sample size may have limited the ability to detect significant differences, leading to inconclusive results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


