{"title":"What's your diagnosis? Circumferential small intestinal mass in a cat","authors":"Cheryl L. Auch, Nutnapong Udomteerasuwat","doi":"10.1111/vcp.13396","DOIUrl":null,"url":null,"abstract":"<p>An 8-year-old, castrated male domestic shorthair cat was presented to their veterinarian to investigate potential causes for vomiting and weight loss (0.45 kg) over the past 9-month period. On a CBC (ProCyte, IDEXX Laboratories), eosinophilia (4860/μL; reference interval: 170–1570) was noted, and a heparinized plasma chemistry panel was unremarkable. Abdominal ultrasound identified a 2.5-cm circumferential, irregular duodenal mass, and fine-needle aspiration biopsies were obtained. The prepared smears were submitted for cytologic evaluation (Figure 1A–D). Additional abnormalities identified via ultrasound included a thickened gallbladder wall, decreased corticomedullary definition in both kidneys and mild mesenteric lymphadenomegaly. The remainder of the abdominal ultrasound evaluation was unremarkable.</p><p>After evaluation of the cytologic specimen, the veterinarian performed an exploratory laparotomy. An approximately 3-cm x 3-cm, duodenal, ulcerated mass was identified immediately aboral to the pyloric sphincter and approximately 5 mm from the sphincter of Oddi. A Billroth I procedure with a choleduodenostomy, and resection was required to obtain adequate margins and reroute the biliary system. Due to the concern for possible mast cell disease, splenectomy and excision of the regional lymph node were also performed, along with an incisional biopsy of the left lateral liver lobe.</p><p>The tissue biopsies of the duodenal mass, spleen, duodenal lymph node and liver were submitted for histologic evaluation. The duodenal mass showed varying densities of plump spindle cells interwoven by collagenous trabeculae extensively affecting the tunica muscularis, submucosa, and mucosa, as appreciated on H&E and Masson's trichrome sections (Figure 2A,B). The spindle cells exhibited basophilic cytoplasm, distinct cell borders, and round vesiculated nuclei with a single prominent nucleolus (Figure 2C). Anisokaryosis was moderate, with 20 mitotic figures in 2.37-mm<sup>2</sup>. The mucosal surface was ulcerated and accompanied by degenerate neutrophils, hemorrhage, and bacterial colonies (Gram-positive cocci and Gram-negative rods). No infectious organisms were detected within the mass on the H&E, Gram, Giemsa or PAS-stained sections. Variable numbers of mast cells, highlighted by toluidine blue stain, and eosinophils were intermixed with the spindle cell population (Figure 2C,D). These findings corresponded with a diagnosis of feline eosinophilic sclerosing fibroplasia.</p><p>The duodenal lymph node biopsy displayed low numbers of eosinophils and histiocytes scattered within the subcapsular and medullary sinuses, consistent with mild, multifocal, eosinophilic lymphadenitis. Histologically, the liver contained multifocal periportal aggregates comprised of a few small lymphocytes, plasma cells, and rare eosinophils, indicating mild, lymphoplasmacytic and eosinophilic periportal hepatitis. The splenic biopsy was histologically normal.</p><p>Feline gastrointestinal eosinophilic sclerosing fibroplasia (FGESF) was first described in 2009 as a unique inflammatory lesion of the feline gastrointestinal tract (stomach to colon) and associated lymph nodes.<span><sup>1</sup></span> Since the condition was originally reported, lesions have been further identified in the rectum,<span><sup>2</sup></span> distant lymph nodes,<span><sup>3</sup></span> nasal cavity,<span><sup>3</sup></span> retroperitoneal space,<span><sup>4</sup></span> liver,<span><sup>5</sup></span> pancreas,<span><sup>6</sup></span> mediastinum,<span><sup>7</sup></span> and mesentery,<span><sup>8</sup></span> which has led to the proposal of the more inclusive term “feline eosinophilic sclerosing fibroplasia (FESF).”<span><sup>3</sup></span> Affected cats typically range in age from 14 weeks to 16 years, with the reported median ages falling between 5 and 8 years.<span><sup>1, 9</sup></span> Neutered males and long-haired cats, particularly the Ragdoll breed, have been disproportionately represented, which may suggest a genetic role.<span><sup>1, 10</sup></span> Clinical signs are often chronic, and presenting complaints include vomiting, diarrhea or constipation, weight loss, decreased appetite, excessive or decreased grooming, and lethargy.<span><sup>9</sup></span> On physical examination, an intra-abdominal mass is often (>85% of cases) palpable.<span><sup>1, 9</sup></span> Clinicopathologic tests may reveal eosinophilia (~50% of cases), anemia (~66% of cases), neutrophilia or neutropenia, monocytosis, lymphocytosis, basophilia, evidence of cholestasis, hypoalbuminemia, and hyperglobulinemia.<span><sup>1, 9</sup></span> Ultrasonographic features are indistinguishable between FESF and neoplasia; therefore, additional diagnostic tests such as fine-needle aspiration and/or biopsy are encouraged.<span><sup>5</sup></span> Grossly, gastrointestinal lesions appear as ulcerated mural masses, as noted in this case.<span><sup>1</sup></span> Lesions beyond the digestive tract can appear as nodules or masses.<span><sup>3</sup></span></p><p>Similar to this case, typical cytologic findings include a proliferation of large, irregular to spindled cells associated with pink extracellular matrix and numerous eosinophils.<span><sup>1</sup></span> Neutrophils with or without intracellular, rod and/or cocci bacteria may also be seen.<span><sup>1</sup></span> Small to intermediate lymphocytes, degranulated mast cells, and plasma cells may be present in low numbers.<span><sup>1</sup></span> The heterogeneity of the cellular components in FESF may pose a diagnostic challenge cytologically, especially if the cytologic specimens only reflect focal areas of the lesion. Cytologic differentials may include sarcomas, mast cell disease, and inflammatory lesions with reactive fibroplasia.<span><sup>2</sup></span> Ultimately, cytology alone often cannot reach a diagnosis of FESF, and histopathologic evaluation of a tissue biopsy is needed to confirm the diagnosis.<span><sup>2</sup></span> However, cytology can still be beneficial to rule out other, more common, neoplasms such as lymphoma or adenocarcinoma. However, FESF lesions can sometimes also pose a diagnostic challenge histologically due to marked mast cell infiltrations, aggregates of dense collagen mimicking osteoid, and variable degrees of mitotic activity and nuclear pleomorphism, which can lead to misdiagnoses such as mast cell tumors, fibrosarcomas, and extraskeletal osteosarcomas.<span><sup>1, 11</sup></span> Discrimination between FESF lesions and sclerosing mast cell tumors can be particularly challenging, and differentiation between the two can be aided by assessment of the mast cell distribution.<span><sup>11</sup></span> The mast cells in FESF lesions are multifocally distributed amongst the other inflammatory cells, while the mast cells in mast cell tumors aggregate in sheets to form a distinct mass.<span><sup>11</sup></span> Histochemical stains such as toluidine blue and Masson's trichrome may be helpful for characterization and confirmation of the diagnosis.<span><sup>11</sup></span> The most consistently described histologic findings include dense collagen trabeculae, numerous large fibroblasts, and many eosinophils.<span><sup>1</sup></span> Intralesional bacteria are also common and can be located within microabscesses and necrotic foci; though in this case, the bacterial organisms were isolated to the ulcerated mucosal surface and not appreciated within the mass.<span><sup>1, 2, 11</sup></span> Giemsa stain, Ziehl-Neelsen stain, Gram Twort's stain, periodic acid-Schiff stain, immunochemistry, and/or fluorescence in situ hybridization have also been used to detect intralesional organisms.<span><sup>1, 11</sup></span></p><p>The pathogenesis of FESF lesions has not been completely elucidated.<span><sup>10</sup></span> It is hypothesized that the eosinophilic inflammation is associated with an inherited dysregulated inflammatory response, similar to eosinophilic granuloma complex.<span><sup>6</sup></span> Chronic inflammation and hypersensitivity responses may predispose cats to FESF due to immunoglobulin E binding with previously encountered antigens and mast cells via the actions of interleukin-5.<span><sup>6</sup></span> Fibrosis may result from an overexuberant reaction to an inflammatory process or antigenic stimulation resulting in exaggerated collagen deposition with collagen type switching observed between mild and more severe lesions.<span><sup>1, 3, 10</sup></span> It is thought that the inflammatory process triggers increased production of transforming growth factor beta-1 and insulin-like growth factor 1 which subsequently induces changes in the fibroblast phenotype.<span><sup>10</sup></span> Chronic antigenic stimulation is suspected to play a role in the development of FESF lesions due to the frequent association with intralesional bacteria or less commonly fungal organisms.<span><sup>9</sup></span> Other proposed mechanisms include dysregulation of eosinophils, dysbiosis, ingestion of foreign material, food hypersensitivities, extracellular endoparasites, or penetrating wounds such as gastrointestinal foreign bodies.<span><sup>6, 10</sup></span> There has been no evidence supporting feline coronavirus or herpesvirus-1 for the development of FESF lesions.<span><sup>11</sup></span> Despite the frequency of intralesional bacteria, administration of antibiotics alone does not appear effective for resolving FESF lesions.<span><sup>3</sup></span> Current treatment protocols are multimodal and typically include a combination of immunosuppressive medications, predominantly corticosteroids, along with surgical debulking or resection, when possible.<span><sup>6, 9</sup></span> Hydrolyzed or selected protein diets have been investigated, though their effectiveness is currently unclear.<span><sup>9</sup></span> The prognosis for cats with FESF is variable and may be guarded to good, depending on the location of the lesion, selected treatment options, and overall response to therapy.<span><sup>4, 9</sup></span></p><p>The authors declare that they have no conflict of interest.</p>","PeriodicalId":23593,"journal":{"name":"Veterinary clinical pathology","volume":"54 S1","pages":"S29-S32"},"PeriodicalIF":1.1000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/vcp.13396","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Veterinary clinical pathology","FirstCategoryId":"97","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/vcp.13396","RegionNum":4,"RegionCategory":"农林科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
An 8-year-old, castrated male domestic shorthair cat was presented to their veterinarian to investigate potential causes for vomiting and weight loss (0.45 kg) over the past 9-month period. On a CBC (ProCyte, IDEXX Laboratories), eosinophilia (4860/μL; reference interval: 170–1570) was noted, and a heparinized plasma chemistry panel was unremarkable. Abdominal ultrasound identified a 2.5-cm circumferential, irregular duodenal mass, and fine-needle aspiration biopsies were obtained. The prepared smears were submitted for cytologic evaluation (Figure 1A–D). Additional abnormalities identified via ultrasound included a thickened gallbladder wall, decreased corticomedullary definition in both kidneys and mild mesenteric lymphadenomegaly. The remainder of the abdominal ultrasound evaluation was unremarkable.
After evaluation of the cytologic specimen, the veterinarian performed an exploratory laparotomy. An approximately 3-cm x 3-cm, duodenal, ulcerated mass was identified immediately aboral to the pyloric sphincter and approximately 5 mm from the sphincter of Oddi. A Billroth I procedure with a choleduodenostomy, and resection was required to obtain adequate margins and reroute the biliary system. Due to the concern for possible mast cell disease, splenectomy and excision of the regional lymph node were also performed, along with an incisional biopsy of the left lateral liver lobe.
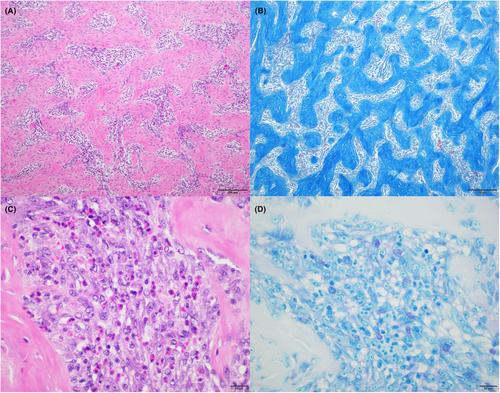
The tissue biopsies of the duodenal mass, spleen, duodenal lymph node and liver were submitted for histologic evaluation. The duodenal mass showed varying densities of plump spindle cells interwoven by collagenous trabeculae extensively affecting the tunica muscularis, submucosa, and mucosa, as appreciated on H&E and Masson's trichrome sections (Figure 2A,B). The spindle cells exhibited basophilic cytoplasm, distinct cell borders, and round vesiculated nuclei with a single prominent nucleolus (Figure 2C). Anisokaryosis was moderate, with 20 mitotic figures in 2.37-mm2. The mucosal surface was ulcerated and accompanied by degenerate neutrophils, hemorrhage, and bacterial colonies (Gram-positive cocci and Gram-negative rods). No infectious organisms were detected within the mass on the H&E, Gram, Giemsa or PAS-stained sections. Variable numbers of mast cells, highlighted by toluidine blue stain, and eosinophils were intermixed with the spindle cell population (Figure 2C,D). These findings corresponded with a diagnosis of feline eosinophilic sclerosing fibroplasia.
The duodenal lymph node biopsy displayed low numbers of eosinophils and histiocytes scattered within the subcapsular and medullary sinuses, consistent with mild, multifocal, eosinophilic lymphadenitis. Histologically, the liver contained multifocal periportal aggregates comprised of a few small lymphocytes, plasma cells, and rare eosinophils, indicating mild, lymphoplasmacytic and eosinophilic periportal hepatitis. The splenic biopsy was histologically normal.
Feline gastrointestinal eosinophilic sclerosing fibroplasia (FGESF) was first described in 2009 as a unique inflammatory lesion of the feline gastrointestinal tract (stomach to colon) and associated lymph nodes.1 Since the condition was originally reported, lesions have been further identified in the rectum,2 distant lymph nodes,3 nasal cavity,3 retroperitoneal space,4 liver,5 pancreas,6 mediastinum,7 and mesentery,8 which has led to the proposal of the more inclusive term “feline eosinophilic sclerosing fibroplasia (FESF).”3 Affected cats typically range in age from 14 weeks to 16 years, with the reported median ages falling between 5 and 8 years.1, 9 Neutered males and long-haired cats, particularly the Ragdoll breed, have been disproportionately represented, which may suggest a genetic role.1, 10 Clinical signs are often chronic, and presenting complaints include vomiting, diarrhea or constipation, weight loss, decreased appetite, excessive or decreased grooming, and lethargy.9 On physical examination, an intra-abdominal mass is often (>85% of cases) palpable.1, 9 Clinicopathologic tests may reveal eosinophilia (~50% of cases), anemia (~66% of cases), neutrophilia or neutropenia, monocytosis, lymphocytosis, basophilia, evidence of cholestasis, hypoalbuminemia, and hyperglobulinemia.1, 9 Ultrasonographic features are indistinguishable between FESF and neoplasia; therefore, additional diagnostic tests such as fine-needle aspiration and/or biopsy are encouraged.5 Grossly, gastrointestinal lesions appear as ulcerated mural masses, as noted in this case.1 Lesions beyond the digestive tract can appear as nodules or masses.3
Similar to this case, typical cytologic findings include a proliferation of large, irregular to spindled cells associated with pink extracellular matrix and numerous eosinophils.1 Neutrophils with or without intracellular, rod and/or cocci bacteria may also be seen.1 Small to intermediate lymphocytes, degranulated mast cells, and plasma cells may be present in low numbers.1 The heterogeneity of the cellular components in FESF may pose a diagnostic challenge cytologically, especially if the cytologic specimens only reflect focal areas of the lesion. Cytologic differentials may include sarcomas, mast cell disease, and inflammatory lesions with reactive fibroplasia.2 Ultimately, cytology alone often cannot reach a diagnosis of FESF, and histopathologic evaluation of a tissue biopsy is needed to confirm the diagnosis.2 However, cytology can still be beneficial to rule out other, more common, neoplasms such as lymphoma or adenocarcinoma. However, FESF lesions can sometimes also pose a diagnostic challenge histologically due to marked mast cell infiltrations, aggregates of dense collagen mimicking osteoid, and variable degrees of mitotic activity and nuclear pleomorphism, which can lead to misdiagnoses such as mast cell tumors, fibrosarcomas, and extraskeletal osteosarcomas.1, 11 Discrimination between FESF lesions and sclerosing mast cell tumors can be particularly challenging, and differentiation between the two can be aided by assessment of the mast cell distribution.11 The mast cells in FESF lesions are multifocally distributed amongst the other inflammatory cells, while the mast cells in mast cell tumors aggregate in sheets to form a distinct mass.11 Histochemical stains such as toluidine blue and Masson's trichrome may be helpful for characterization and confirmation of the diagnosis.11 The most consistently described histologic findings include dense collagen trabeculae, numerous large fibroblasts, and many eosinophils.1 Intralesional bacteria are also common and can be located within microabscesses and necrotic foci; though in this case, the bacterial organisms were isolated to the ulcerated mucosal surface and not appreciated within the mass.1, 2, 11 Giemsa stain, Ziehl-Neelsen stain, Gram Twort's stain, periodic acid-Schiff stain, immunochemistry, and/or fluorescence in situ hybridization have also been used to detect intralesional organisms.1, 11
The pathogenesis of FESF lesions has not been completely elucidated.10 It is hypothesized that the eosinophilic inflammation is associated with an inherited dysregulated inflammatory response, similar to eosinophilic granuloma complex.6 Chronic inflammation and hypersensitivity responses may predispose cats to FESF due to immunoglobulin E binding with previously encountered antigens and mast cells via the actions of interleukin-5.6 Fibrosis may result from an overexuberant reaction to an inflammatory process or antigenic stimulation resulting in exaggerated collagen deposition with collagen type switching observed between mild and more severe lesions.1, 3, 10 It is thought that the inflammatory process triggers increased production of transforming growth factor beta-1 and insulin-like growth factor 1 which subsequently induces changes in the fibroblast phenotype.10 Chronic antigenic stimulation is suspected to play a role in the development of FESF lesions due to the frequent association with intralesional bacteria or less commonly fungal organisms.9 Other proposed mechanisms include dysregulation of eosinophils, dysbiosis, ingestion of foreign material, food hypersensitivities, extracellular endoparasites, or penetrating wounds such as gastrointestinal foreign bodies.6, 10 There has been no evidence supporting feline coronavirus or herpesvirus-1 for the development of FESF lesions.11 Despite the frequency of intralesional bacteria, administration of antibiotics alone does not appear effective for resolving FESF lesions.3 Current treatment protocols are multimodal and typically include a combination of immunosuppressive medications, predominantly corticosteroids, along with surgical debulking or resection, when possible.6, 9 Hydrolyzed or selected protein diets have been investigated, though their effectiveness is currently unclear.9 The prognosis for cats with FESF is variable and may be guarded to good, depending on the location of the lesion, selected treatment options, and overall response to therapy.4, 9
The authors declare that they have no conflict of interest.
期刊介绍:
Veterinary Clinical Pathology is the official journal of the American Society for Veterinary Clinical Pathology (ASVCP) and the European Society of Veterinary Clinical Pathology (ESVCP). The journal''s mission is to provide an international forum for communication and discussion of scientific investigations and new developments that advance the art and science of laboratory diagnosis in animals. Veterinary Clinical Pathology welcomes original experimental research and clinical contributions involving domestic, laboratory, avian, and wildlife species in the areas of hematology, hemostasis, immunopathology, clinical chemistry, cytopathology, surgical pathology, toxicology, endocrinology, laboratory and analytical techniques, instrumentation, quality assurance, and clinical pathology education.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


