A Ruiz-Hernández, E González-Arnaiz, I González-Puente, J Tejada-García, I Beltrán-Rodríguez, L A García Tuñón-Villaluenga, A Pérez-Álvarez, P González-Feito, B Villarrubia-González, J Barrutia-Yovera, M D Ballesteros-Pomar
{"title":"[Glycemic management in the stroke unit and its relationship with morbidity and mortality].","authors":"A Ruiz-Hernández, E González-Arnaiz, I González-Puente, J Tejada-García, I Beltrán-Rodríguez, L A García Tuñón-Villaluenga, A Pérez-Álvarez, P González-Feito, B Villarrubia-González, J Barrutia-Yovera, M D Ballesteros-Pomar","doi":"10.33588/rn.7908.2023337","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To determine the treatment of hyperglycemia in the stroke unit, and to compare the morbidity and mortality of patients treated with an intravenous (iv) insulin therapy protocol compared to subcutaneous (sc) insulin when reaching glycemia levels of = 155 mg/dL.</p><p><strong>Patients and methods: </strong>We performed a prospective observational study of patients admitted to our stroke unit between July and October 2022. Demographic, glycemic and prognostic variables were collected. Glycemic variability was defined as the standard deviation (SD) of the mean individual glycemia during the first 24-72 hours. Acute complications during admission and mortality at discharge and at 3 months were determined. The variables were analysed by subgroup according to the insulin regime in patients with type 2 diabetes mellitus (DM2) or stress hyperglycemia.</p><p><strong>Results: </strong>The sample consisted of 181 patients, of whom 63.5% were male, with a mean age of 74.2 (SD: 11.6) years. 25.4% required insulin due to glycemia = 155 mg/dL (18 patients iv and 28 sc). 31.5% had DM2 (82.6% of the group receiving insulin and 14% of group without insulin). The group receiving insulin presented higher levels of glycemic variability, at 33.3 (SD: 21.7) mg/dL vs. 11.7 (SD: 7) mg/dL (p < 0.01), more acute complications (43.5% vs. 19.2%; p < 0.01) and higher mortality at 3 months (19.5% vs. 6.6%; p = 0.04) than the group without insulin, and no differences were observed between the type of insulin regime in the subgroups with DM2 or stress hyperglycemia.</p><p><strong>Conclusions: </strong>The patients with glycemia = 155 mg/dL presented higher levels of glycemic variability, acute complications and mortality at 3 months, and no differences were observed in the type of insulin regime, regardless of whether they had DM2.</p>","PeriodicalId":21281,"journal":{"name":"Revista de neurologia","volume":"79 8","pages":"209-215"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11605905/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista de neurologia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.33588/rn.7908.2023337","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: To determine the treatment of hyperglycemia in the stroke unit, and to compare the morbidity and mortality of patients treated with an intravenous (iv) insulin therapy protocol compared to subcutaneous (sc) insulin when reaching glycemia levels of = 155 mg/dL.
Patients and methods: We performed a prospective observational study of patients admitted to our stroke unit between July and October 2022. Demographic, glycemic and prognostic variables were collected. Glycemic variability was defined as the standard deviation (SD) of the mean individual glycemia during the first 24-72 hours. Acute complications during admission and mortality at discharge and at 3 months were determined. The variables were analysed by subgroup according to the insulin regime in patients with type 2 diabetes mellitus (DM2) or stress hyperglycemia.
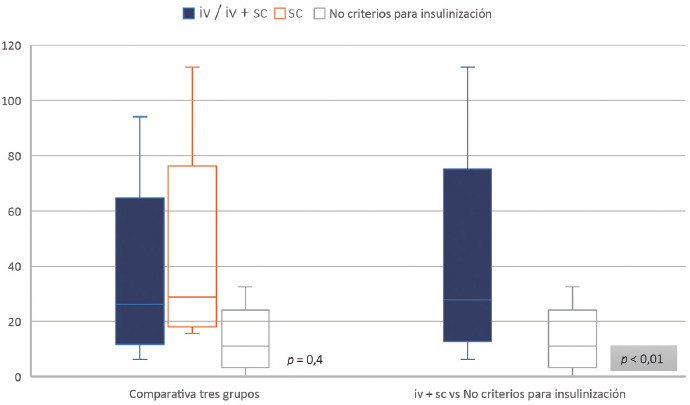
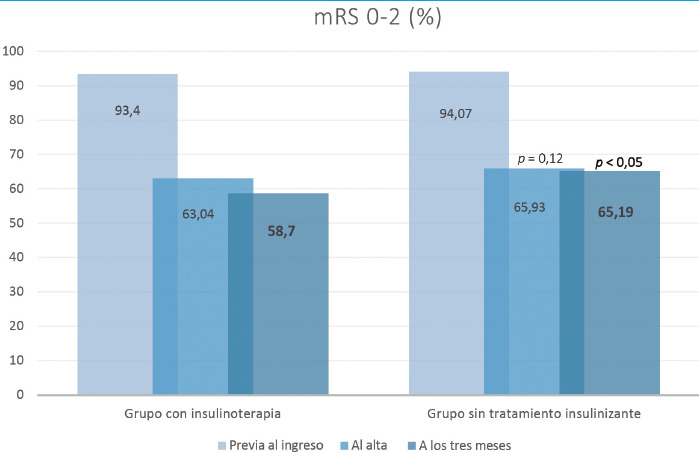
Results: The sample consisted of 181 patients, of whom 63.5% were male, with a mean age of 74.2 (SD: 11.6) years. 25.4% required insulin due to glycemia = 155 mg/dL (18 patients iv and 28 sc). 31.5% had DM2 (82.6% of the group receiving insulin and 14% of group without insulin). The group receiving insulin presented higher levels of glycemic variability, at 33.3 (SD: 21.7) mg/dL vs. 11.7 (SD: 7) mg/dL (p < 0.01), more acute complications (43.5% vs. 19.2%; p < 0.01) and higher mortality at 3 months (19.5% vs. 6.6%; p = 0.04) than the group without insulin, and no differences were observed between the type of insulin regime in the subgroups with DM2 or stress hyperglycemia.
Conclusions: The patients with glycemia = 155 mg/dL presented higher levels of glycemic variability, acute complications and mortality at 3 months, and no differences were observed in the type of insulin regime, regardless of whether they had DM2.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


