Technical Approaches for Coil Embolization of Unruptured Small Anterior Choroidal Artery Aneurysms: A Focus on Anatomical Flow Preservation of the Anterior Choroidal Artery.
{"title":"Technical Approaches for Coil Embolization of Unruptured Small Anterior Choroidal Artery Aneurysms: A Focus on Anatomical Flow Preservation of the Anterior Choroidal Artery.","authors":"Dae Chul Suh","doi":"10.5469/neuroint.2024.00353","DOIUrl":null,"url":null,"abstract":"<p><p>The anterior choroidal artery (AChA) supplies the corticospinal tract related to the motor function of the upper and lower limbs. Aneurysms arising at the AChA are not common and exhibit various patterns of involvement of the AChA. Hence, managing an AChA aneurysm poses a high risk of neurological deficits. We report technical issues related to the outcome of coil embolization for unruptured AChA aneurysms. We obtained Institutional Review Board approval for this study. In the past 2 years, 18 consecutive patients (6 males and 12 females, aged 32-68) with unruptured AChA aneurysms were treated using embolization. We present technical details, pre- and post-procedural patient statuses, angiographic outcomes, and recurrence during a mean follow-up period of 12 months (range 3-25). The patients with AChA (n=18) underwent stent-assisted coiling (n=14), coiling (n=2), or stenting only (n=2). The technical strategy for aneurysm embolization included a low-lying approach into the aneurysm, stent-strut abutting (protecting) coil framing to block inflow and avoid compromising AChA flow, and direct intra-aneurysmal angiography via a microcatheter. Angiographic results showed complete occlusion (n=11), neck remnant (n=5), and sac remnant (n=2). During the follow-up, there were 2 recurrences, and 1 of them required a re-procedure. All patients showed no change in clinical status (modified Rankin scale score=0) and did not experience any ischemic or hemorrhagic events during the follow-up period. AChA aneurysms can be managed through embolization using various techniques. Such technical concepts may enhance the safety and improve the outcomes of AChA aneurysm embolization.</p>","PeriodicalId":19140,"journal":{"name":"Neurointervention","volume":" ","pages":"162-168"},"PeriodicalIF":1.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11540482/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurointervention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5469/neuroint.2024.00353","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/15 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
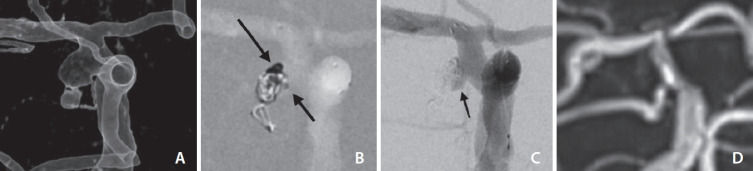
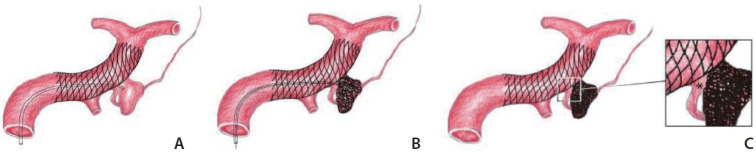
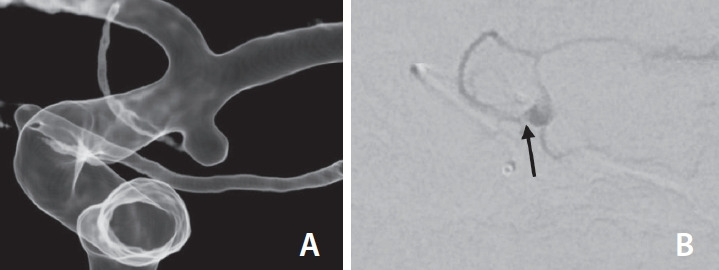
The anterior choroidal artery (AChA) supplies the corticospinal tract related to the motor function of the upper and lower limbs. Aneurysms arising at the AChA are not common and exhibit various patterns of involvement of the AChA. Hence, managing an AChA aneurysm poses a high risk of neurological deficits. We report technical issues related to the outcome of coil embolization for unruptured AChA aneurysms. We obtained Institutional Review Board approval for this study. In the past 2 years, 18 consecutive patients (6 males and 12 females, aged 32-68) with unruptured AChA aneurysms were treated using embolization. We present technical details, pre- and post-procedural patient statuses, angiographic outcomes, and recurrence during a mean follow-up period of 12 months (range 3-25). The patients with AChA (n=18) underwent stent-assisted coiling (n=14), coiling (n=2), or stenting only (n=2). The technical strategy for aneurysm embolization included a low-lying approach into the aneurysm, stent-strut abutting (protecting) coil framing to block inflow and avoid compromising AChA flow, and direct intra-aneurysmal angiography via a microcatheter. Angiographic results showed complete occlusion (n=11), neck remnant (n=5), and sac remnant (n=2). During the follow-up, there were 2 recurrences, and 1 of them required a re-procedure. All patients showed no change in clinical status (modified Rankin scale score=0) and did not experience any ischemic or hemorrhagic events during the follow-up period. AChA aneurysms can be managed through embolization using various techniques. Such technical concepts may enhance the safety and improve the outcomes of AChA aneurysm embolization.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


