Sairi Zhang, Kaersti L Rickels, Vignesh Krishnan, Sami H Uwaydat
{"title":"Persistent syphilitic ocular manifestations despite treatment: a case series.","authors":"Sairi Zhang, Kaersti L Rickels, Vignesh Krishnan, Sami H Uwaydat","doi":"10.1186/s12348-024-00435-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Penicillin has remained the most effective treatment for syphilis for several decades. Syphilitic retinal manifestations may persist following treatment and cause visual problems. In this case series, we describe three syphilis patients with persistent posterior segment manifestations due to chronic inflammation, incomplete treatment, and reinfection.</p><p><strong>Case series: </strong>Recommended initial treatment for all patients was 14 days of intravenous penicillin. Oral prednisone was added 48 h after initiation of penicillin therapy. Case 1: A 48-year-old female presented with gradual vision loss for two months. Fundus imaging revealed syphilitic outer retinopathy (SOR), papillitis, and acute syphilitic posterior placoid chorioretinopathy (ASPPC). After treatment, she had persistent cystoid macular edema (CME) and was treated with intravitreal triamcinolone injections and ketorolac drops.</p><p><strong>Case 2: </strong>A 24-year-old male presented with sudden vision loss for two days. On imaging, he had ASPPC, papillitis, and SOR. IV penicillin treatment was given for 10 days only. He had persistent SOR and was retreated with doxycycline and prednisone. Case 3: A 52-year-old male presented with eye pain and visual loss for one week. There was evidence of ASPPC and papillitis on imaging. One month after treatment, he had persistent papillitis and was restarted on oral prednisone. One year later, he was found to have recurrent ASPPC and was confirmed to be reinfected with syphilis, for which he was retreated.</p><p><strong>Conclusion: </strong>When treating persistent syphilitic ocular manifestations, we recommend checking that the penicillin treatment was complete and the RPR titers are declining. If both hold true, then the affected eye should be treated with anti-inflammatory therapy. Other factors that contribute to poor visual prognosis include treatment delay, poor initial visual acuity, macular edema, and HIV coinfection.</p>","PeriodicalId":16600,"journal":{"name":"Journal of Ophthalmic Inflammation and Infection","volume":"14 1","pages":"53"},"PeriodicalIF":2.3000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11489380/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ophthalmic Inflammation and Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12348-024-00435-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Penicillin has remained the most effective treatment for syphilis for several decades. Syphilitic retinal manifestations may persist following treatment and cause visual problems. In this case series, we describe three syphilis patients with persistent posterior segment manifestations due to chronic inflammation, incomplete treatment, and reinfection.
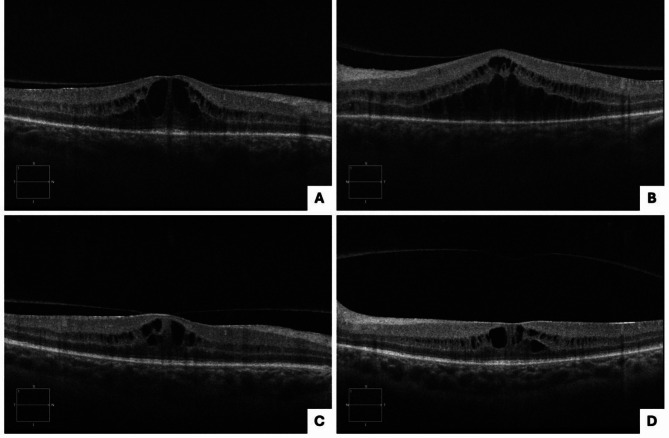
Case series: Recommended initial treatment for all patients was 14 days of intravenous penicillin. Oral prednisone was added 48 h after initiation of penicillin therapy. Case 1: A 48-year-old female presented with gradual vision loss for two months. Fundus imaging revealed syphilitic outer retinopathy (SOR), papillitis, and acute syphilitic posterior placoid chorioretinopathy (ASPPC). After treatment, she had persistent cystoid macular edema (CME) and was treated with intravitreal triamcinolone injections and ketorolac drops.
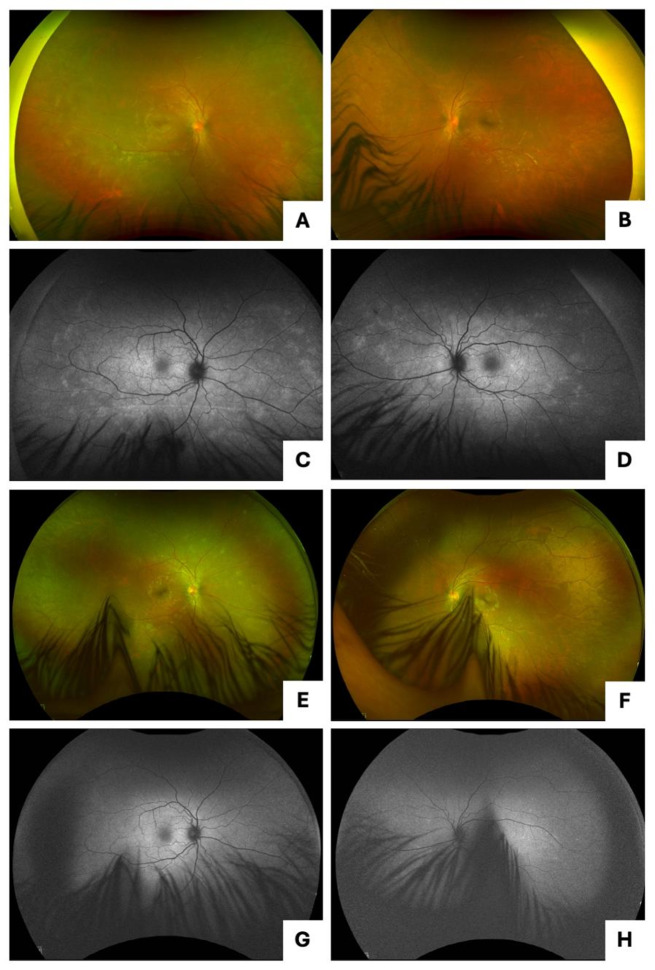
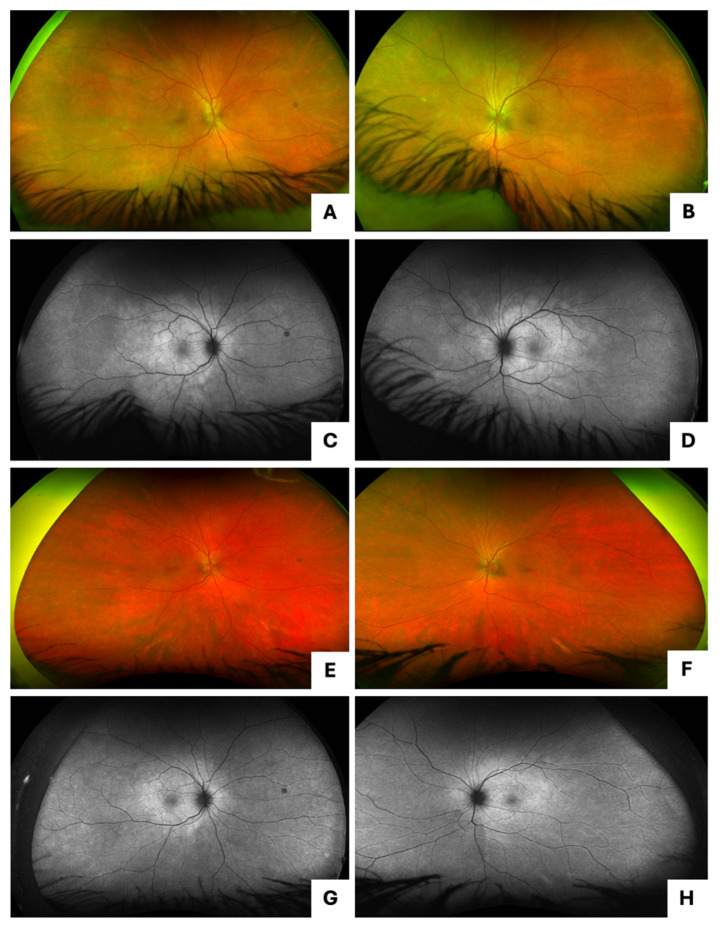
Case 2: A 24-year-old male presented with sudden vision loss for two days. On imaging, he had ASPPC, papillitis, and SOR. IV penicillin treatment was given for 10 days only. He had persistent SOR and was retreated with doxycycline and prednisone. Case 3: A 52-year-old male presented with eye pain and visual loss for one week. There was evidence of ASPPC and papillitis on imaging. One month after treatment, he had persistent papillitis and was restarted on oral prednisone. One year later, he was found to have recurrent ASPPC and was confirmed to be reinfected with syphilis, for which he was retreated.
Conclusion: When treating persistent syphilitic ocular manifestations, we recommend checking that the penicillin treatment was complete and the RPR titers are declining. If both hold true, then the affected eye should be treated with anti-inflammatory therapy. Other factors that contribute to poor visual prognosis include treatment delay, poor initial visual acuity, macular edema, and HIV coinfection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


