Rahul Bhatnagar, Kristian Berge, Arne Didrik Høiseth, Torbjørn Omland, Magnus Nakrem Lyngbakken, Helge Røsjø
{"title":"Associations between Chest Pain, Diagnosis, and Clinical Outcome in Patients Hospitalized with Acute Dyspnea: Data from the ACE 2 Study.","authors":"Rahul Bhatnagar, Kristian Berge, Arne Didrik Høiseth, Torbjørn Omland, Magnus Nakrem Lyngbakken, Helge Røsjø","doi":"10.1159/000541897","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients hospitalized due to dyspnea sometimes also report concomitant chest pain. Whether co-existing chest pain in patients with acute dyspnea associates with specific diagnosis and clinical outcome is not known.</p><p><strong>Method: </strong>We included 313 patients admitted to Akershus University Hospital with acute dyspnea and asked the patients directly on hospital admission whether they had experienced chest pain during the last 24 h. We examined the associations between chest pain and (1) diagnosis of the index hospitalization and (2) clinical outcome during follow-up. The diagnosis for the index hospitalization was adjudicated as acute heart failure (HF) or non-HF etiology of acute dyspnea by two experts working independently. Non-HF patients were further sub-grouped into chronic obstructive pulmonary disease (COPD) or non-COPD etiology.</p><p><strong>Results: </strong>In total, 143 patients were admitted with acute HF (46% of the population), 83 patients with COPD (26% of the population), and 87 patients with non-HF, non-COPD-related dyspnea (28% of the population). Ninety-six patients (31%) with acute dyspnea reported chest pain during the last 24 h prior to hospital admission. The prevalence of chest pain was not statistically different for patients who were hospitalized with acute HF (n = 42, 44%), acute exacerbation of COPD (n = 22, 23%), or non-HF, non-COPD-related dyspnea (n = 32, 33%), p > 0.05 for all comparisons between groups. During median of 823 days follow-up, 114 patients died (36%). Patients with dyspnea and concomitant chest pain did not have different outcome compared to patients with dyspnea and no chest pain (log-rank test: p = 0.09). Chest pain prior to admission was neither associated with all-cause mortality in any of the adjudicated diagnosis groups.</p><p><strong>Conclusions: </strong>Chest pain was reported in 31% of patients hospitalized with acute dyspnea but the prevalence did not differ according to adjudicated diagnosis. Patients with dyspnea and chest pain did not have worse outcome compared to patients with dyspnea and no chest pain.</p>","PeriodicalId":9391,"journal":{"name":"Cardiology","volume":" ","pages":"233-242"},"PeriodicalIF":1.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136596/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000541897","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Patients hospitalized due to dyspnea sometimes also report concomitant chest pain. Whether co-existing chest pain in patients with acute dyspnea associates with specific diagnosis and clinical outcome is not known.
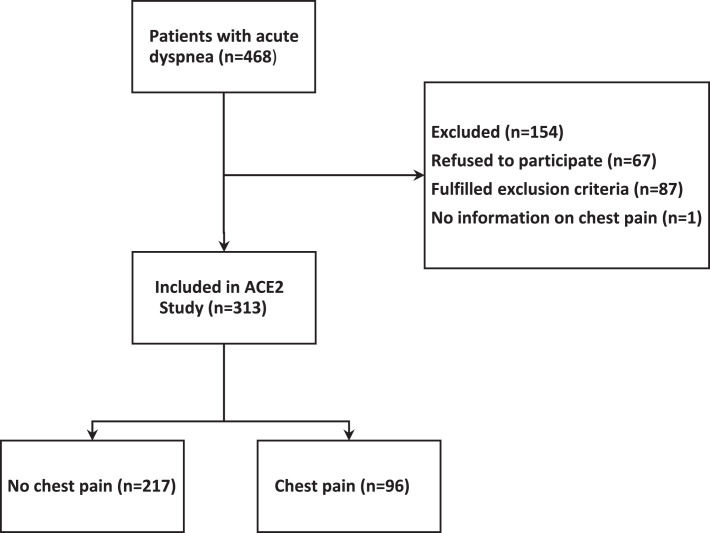
Method: We included 313 patients admitted to Akershus University Hospital with acute dyspnea and asked the patients directly on hospital admission whether they had experienced chest pain during the last 24 h. We examined the associations between chest pain and (1) diagnosis of the index hospitalization and (2) clinical outcome during follow-up. The diagnosis for the index hospitalization was adjudicated as acute heart failure (HF) or non-HF etiology of acute dyspnea by two experts working independently. Non-HF patients were further sub-grouped into chronic obstructive pulmonary disease (COPD) or non-COPD etiology.
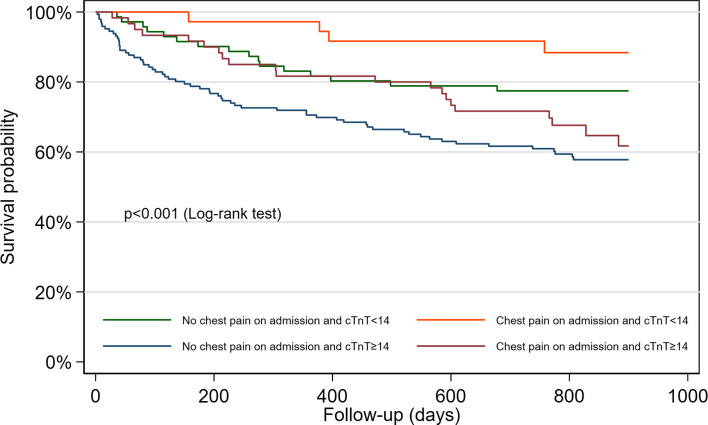
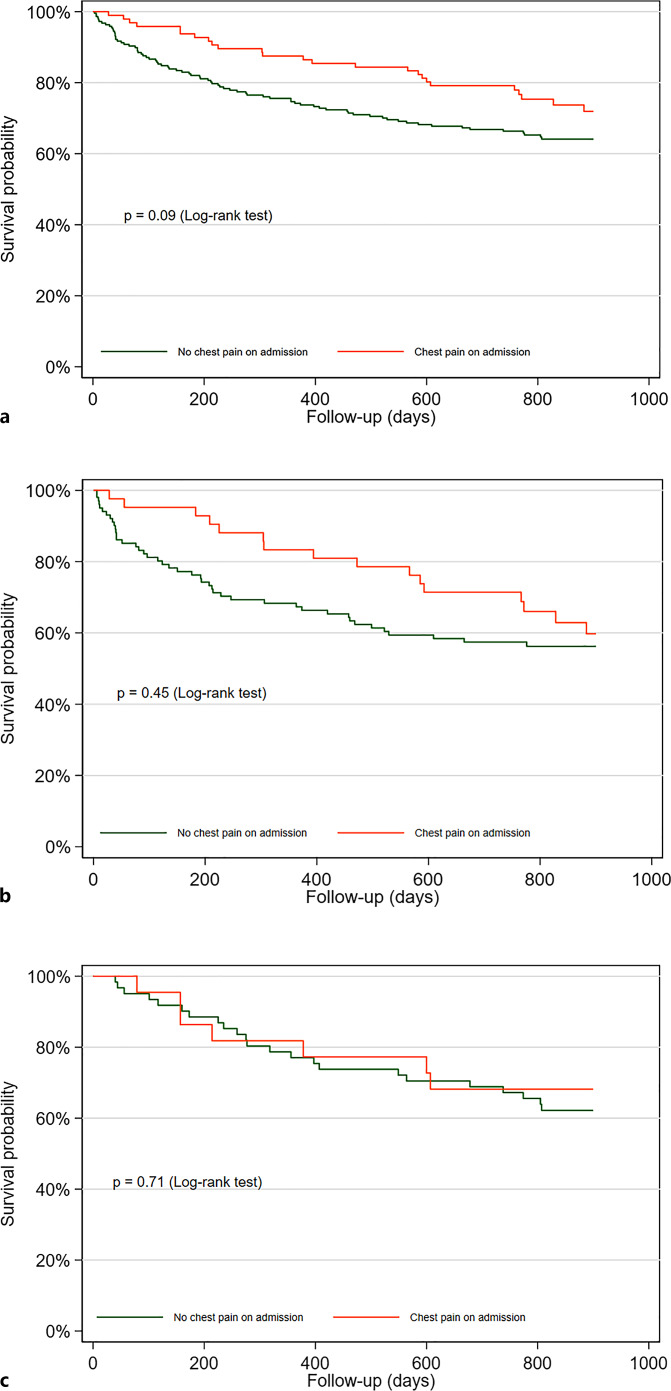
Results: In total, 143 patients were admitted with acute HF (46% of the population), 83 patients with COPD (26% of the population), and 87 patients with non-HF, non-COPD-related dyspnea (28% of the population). Ninety-six patients (31%) with acute dyspnea reported chest pain during the last 24 h prior to hospital admission. The prevalence of chest pain was not statistically different for patients who were hospitalized with acute HF (n = 42, 44%), acute exacerbation of COPD (n = 22, 23%), or non-HF, non-COPD-related dyspnea (n = 32, 33%), p > 0.05 for all comparisons between groups. During median of 823 days follow-up, 114 patients died (36%). Patients with dyspnea and concomitant chest pain did not have different outcome compared to patients with dyspnea and no chest pain (log-rank test: p = 0.09). Chest pain prior to admission was neither associated with all-cause mortality in any of the adjudicated diagnosis groups.
Conclusions: Chest pain was reported in 31% of patients hospitalized with acute dyspnea but the prevalence did not differ according to adjudicated diagnosis. Patients with dyspnea and chest pain did not have worse outcome compared to patients with dyspnea and no chest pain.
期刊介绍:
''Cardiology'' features first reports on original clinical, preclinical and fundamental research as well as ''Novel Insights from Clinical Experience'' and topical comprehensive reviews in selected areas of cardiovascular disease. ''Editorial Comments'' provide a critical but positive evaluation of a recent article. Papers not only describe but offer critical appraisals of new developments in non-invasive and invasive diagnostic methods and in pharmacologic, nutritional and mechanical/surgical therapies. Readers are thus kept informed of current strategies in the prevention, recognition and treatment of heart disease. Special sections in a variety of subspecialty areas reinforce the journal''s value as a complete record of recent progress for all cardiologists, internists, cardiac surgeons, clinical physiologists, pharmacologists and professionals in other areas of medicine interested in current activity in cardiovascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


