Spinal Adhesive Arachnoidopathy, the Disorder More Than Simply Adhesive Arachnoiditis: A Comprehensive Systematic Review of 510 Cases
Abstract
Background
Spinal adhesive arachnoidopathy (SAA) is a chronic pathology associated with persistent inflammatory responses in the arachnoid. Adhesive arachnoiditis (AA) is one of the major forms of SAA, with accompanying secondary complications. Therefore, we aimed to systematically review both clinical and animal model studies related to SAA to gain a deeper understanding of this unique pathology.
Methods
A literature search was conducted in PubMed, EMBASE, and Cochrane Library databases to retrieve relevant publications up to October 2022. Clinical manifestations, etiologies, imaging modalities, treatments, and prognosis in patients with SAA were collected. Data from animal experiments related to SAA were also extracted.
Results
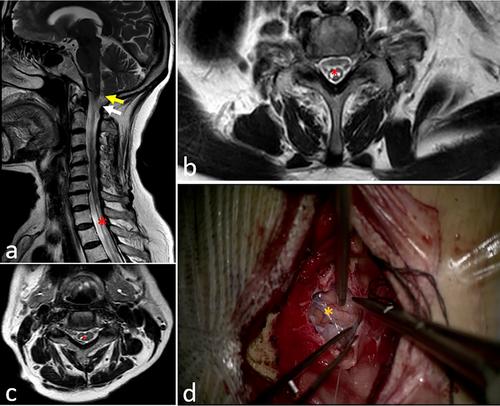
A total of 176 studies, including 147 clinical and 29 animal model studies, with a total of 510 patients were enrolled in this study. Pain (37.5%), abnormal nerve sensations (39.58%), and abnormal motor function (78.75%) were the top three common symptoms of SAA. Major etiologies included trauma (22.7%), infection (17.73%), surgery (15.37%), and hemorrhage (13.48%). MRI was widely used to confirm the diagnosis. AA could be involved in cervical (96/606, 15.84%), thoracic (297/606, 49.01%), lumbar (174/606, 28.71%), and sacrococcygeal (39/606, 6.44%) vertebral segments. Patients with AA in cervical segments had a higher post-surgery recovery rate (p = 0.016) compared to that of other segments. The common pathological diagnoses of SAA were AA (80.82%), AA combined with arachnoid cyst (12.79%), arachnoid calcification/scars (3.43%), and arachnoid web/fibrosis (2.97%). Patients with AA were more likely to develop syringomyelia, compared with patients with other forms of SAA (p < 0.001). Animal studies mainly focused on new AA therapeutic agents (n = 14), the pathomechanism of AA (n = 14), and the development of new MRI sequences for improved diagnosis (n = 1).
Conclusions
The pathological consequences of SAA are more complex than AA and manifest in different forms, such as AA combined with arachnoid cyst, arachnoid calcification/scars, and arachnoid web/fibrosis. In many instances, AA was associated with secondary syringomyelia. Unspecific clinical manifestations of SAA may easily lead to misdiagnosis and missed diagnosis. Although SAA may result from multiple etiologies, including spinal trauma, meningitis, spinal surgery, and hemorrhage, the pathogenesis and treatment of SAA have still not been standardized.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


