Roland H. Stimson, Mark W. J. Strachan, Anna R. Dover, Rohana J. Wright, Shareen Forbes, Gayle McRobert, Fraser W. Gibb
{"title":"Outcomes after 1 year in adults using Omnipod 5: Real-world data from a UK diabetes centre","authors":"Roland H. Stimson, Mark W. J. Strachan, Anna R. Dover, Rohana J. Wright, Shareen Forbes, Gayle McRobert, Fraser W. Gibb","doi":"10.1111/dme.15453","DOIUrl":null,"url":null,"abstract":"<p>Despite substantial advances in diabetes care over the previous decade, only a minority of people with type 1 diabetes achieve an HbA1c <53 mmol/mol.<span><sup>1</sup></span> Automated insulin delivery (AID) systems have consistently demonstrated efficacy in reducing HbA1c.<span><sup>2</sup></span> Omnipod 5 (Insulet Corp) is a tubeless AID system which was launched in the United Kingdom in 2023. Here, we report the first 1-year CGM, HbA1c and weight outcomes in people using Omnipod 5, under routine clinical care, in the United Kingdom.</p><p>This was a prospective, observational assessment based in a single Scottish centre which provides diabetes care for approximately 5000 adults with type 1 diabetes. As a service evaluation of routinely collected data, this project did not require ethical approval. We included all adults who transitioned from Omnipod DASH (standalone CSII) to Omnipod 5 (hybrid closed loop with Dexcom G6 CGM) between June and August 2023. Data were obtained from the electronic health record (SCI-Diabetes), LibreView, Dexcom Clarity and Glooko.</p><p>Paired CGM data were available in 45/50 (90 days prior to Omnipod 5 and 90 days after 1 year of use) and paired HbA1c data were available in 41/50 (measured at a median 200 days [202–336] after OP5 commencement). CGM metrics reported are consistent with those described in the international consensus document.<span><sup>3</sup></span> Paired weight data were available in 28/50 (median 308 days after OP5 commencement [244–370]). Results are presented as median (IQR). Paired data were compared with Wilcoxon signed rank tests and correlations were assessed by Spearman correlation coefficient. <i>p</i> <0.05 were considered statistically significant. Statistical analyses were performed using R Studio.</p><p>Median age was 42 years (IQR: 30–53), duration of diabetes was 24 years (13–34) and 64% were female. Baseline HbA1c was 69 mmol/mol (61–75) and 22% had an HbA1c <58 mmol/mol. Thirty-eight per cent had BMI >30 kg/m<sup>2</sup>. Fifty-nine per cent were predominantly using the lowest glucose target (6.1 mM) at the end of follow-up and median time in auto mode was 94% (91–99).</p><p>In those with paired HbA1c data, median baseline HbA1c was 70 mmol/mol (63–76) and fell to 58 mmol/mol (52–63) during Omnipod 5 use (<i>p</i> < 0.001). Data summarising CGM changes are presented in the figure (Figure 1), including a change in TIR from 42% (33–58) to 60% (53–68, <i>p</i> < 0.001). GMI fell from 66 mmol/mol (57–70) to 58 mmol/mol (54–62, <i>p</i> < 0.001) and coefficient of variation for glucose fell from 37% (34–42) to 34% (32–38, <i>p</i> = 0.009). Change in TIR at 1 year was strongly negatively correlated with baseline TIR (<i>R</i> −0.581, <i>p</i> < 0.001). Percentage of insulin delivered as bolus was negatively correlated with increase in TIR (<i>R</i> −0.518, <i>p</i> < 0.001). Age, sex and socio-economic deprivation were not associated with TIR response to Omnipod 5.</p><p>Median weight change was +2.3 kg (−1.3 to 3.8) or + 3.0% of baseline weight (−1.6 to 5.2). Weight change was not associated with change in HbA1c (<i>R</i> 0.115, <i>p</i> = 0.560) or TIR (<i>R</i> −0.101, <i>p</i> = 0.607).</p><p>We have shown that Omnipod 5 is associated with clinically important improvement in TIR with no increase in TBR. Our cohort differs from other evaluations of Omnipod 5<span><sup>4, 5</sup></span> as the baseline HbA1c of participants was relatively high. Those with lowest TIR (highest HbA1c) are most likely to experience substantial increases in TIR when converting from standalone CSII to Omnipod 5. Individuals where bolus insulin was lowest (in relation to basal insulin) experienced the largest improvements in TIR; suggesting the system is effective in those who have historically delivered insufficient insulin doses at mealtimes. Reassuringly, weight gain was typically modest and not associated with improvements in HbA1c or TIR. This is the first real-world assessment of 1-year outcomes with Omnipod 5 in the United Kingdom and attests to the durability of improvements observed shortly after commencement.</p><p>No funding source to report.</p><p>FWG has received speaker fees from Abbott, Dexcom and Insulet. ARD has received speaker fees from Abbott.</p>","PeriodicalId":11251,"journal":{"name":"Diabetic Medicine","volume":"41 12","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-10-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dme.15453","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetic Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/dme.15453","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Despite substantial advances in diabetes care over the previous decade, only a minority of people with type 1 diabetes achieve an HbA1c <53 mmol/mol.1 Automated insulin delivery (AID) systems have consistently demonstrated efficacy in reducing HbA1c.2 Omnipod 5 (Insulet Corp) is a tubeless AID system which was launched in the United Kingdom in 2023. Here, we report the first 1-year CGM, HbA1c and weight outcomes in people using Omnipod 5, under routine clinical care, in the United Kingdom.
This was a prospective, observational assessment based in a single Scottish centre which provides diabetes care for approximately 5000 adults with type 1 diabetes. As a service evaluation of routinely collected data, this project did not require ethical approval. We included all adults who transitioned from Omnipod DASH (standalone CSII) to Omnipod 5 (hybrid closed loop with Dexcom G6 CGM) between June and August 2023. Data were obtained from the electronic health record (SCI-Diabetes), LibreView, Dexcom Clarity and Glooko.
Paired CGM data were available in 45/50 (90 days prior to Omnipod 5 and 90 days after 1 year of use) and paired HbA1c data were available in 41/50 (measured at a median 200 days [202–336] after OP5 commencement). CGM metrics reported are consistent with those described in the international consensus document.3 Paired weight data were available in 28/50 (median 308 days after OP5 commencement [244–370]). Results are presented as median (IQR). Paired data were compared with Wilcoxon signed rank tests and correlations were assessed by Spearman correlation coefficient. p <0.05 were considered statistically significant. Statistical analyses were performed using R Studio.
Median age was 42 years (IQR: 30–53), duration of diabetes was 24 years (13–34) and 64% were female. Baseline HbA1c was 69 mmol/mol (61–75) and 22% had an HbA1c <58 mmol/mol. Thirty-eight per cent had BMI >30 kg/m2. Fifty-nine per cent were predominantly using the lowest glucose target (6.1 mM) at the end of follow-up and median time in auto mode was 94% (91–99).
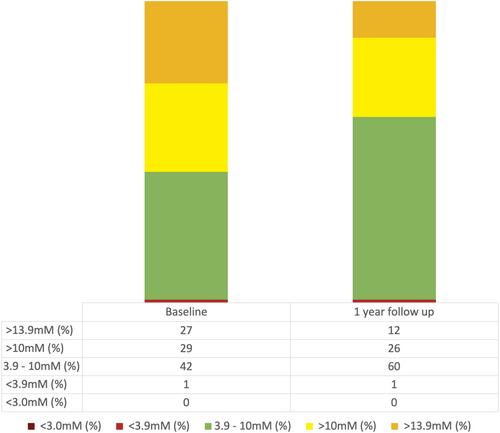
In those with paired HbA1c data, median baseline HbA1c was 70 mmol/mol (63–76) and fell to 58 mmol/mol (52–63) during Omnipod 5 use (p < 0.001). Data summarising CGM changes are presented in the figure (Figure 1), including a change in TIR from 42% (33–58) to 60% (53–68, p < 0.001). GMI fell from 66 mmol/mol (57–70) to 58 mmol/mol (54–62, p < 0.001) and coefficient of variation for glucose fell from 37% (34–42) to 34% (32–38, p = 0.009). Change in TIR at 1 year was strongly negatively correlated with baseline TIR (R −0.581, p < 0.001). Percentage of insulin delivered as bolus was negatively correlated with increase in TIR (R −0.518, p < 0.001). Age, sex and socio-economic deprivation were not associated with TIR response to Omnipod 5.
Median weight change was +2.3 kg (−1.3 to 3.8) or + 3.0% of baseline weight (−1.6 to 5.2). Weight change was not associated with change in HbA1c (R 0.115, p = 0.560) or TIR (R −0.101, p = 0.607).
We have shown that Omnipod 5 is associated with clinically important improvement in TIR with no increase in TBR. Our cohort differs from other evaluations of Omnipod 54, 5 as the baseline HbA1c of participants was relatively high. Those with lowest TIR (highest HbA1c) are most likely to experience substantial increases in TIR when converting from standalone CSII to Omnipod 5. Individuals where bolus insulin was lowest (in relation to basal insulin) experienced the largest improvements in TIR; suggesting the system is effective in those who have historically delivered insufficient insulin doses at mealtimes. Reassuringly, weight gain was typically modest and not associated with improvements in HbA1c or TIR. This is the first real-world assessment of 1-year outcomes with Omnipod 5 in the United Kingdom and attests to the durability of improvements observed shortly after commencement.
No funding source to report.
FWG has received speaker fees from Abbott, Dexcom and Insulet. ARD has received speaker fees from Abbott.
期刊介绍:
Diabetic Medicine, the official journal of Diabetes UK, is published monthly simultaneously, in print and online editions.
The journal publishes a range of key information on all clinical aspects of diabetes mellitus, ranging from human genetic studies through clinical physiology and trials to diabetes epidemiology. We do not publish original animal or cell culture studies unless they are part of a study of clinical diabetes involving humans. Categories of publication include research articles, reviews, editorials, commentaries, and correspondence. All material is peer-reviewed.
We aim to disseminate knowledge about diabetes research with the goal of improving the management of people with diabetes. The journal therefore seeks to provide a forum for the exchange of ideas between clinicians and researchers worldwide. Topics covered are of importance to all healthcare professionals working with people with diabetes, whether in primary care or specialist services.
Surplus generated from the sale of Diabetic Medicine is used by Diabetes UK to know diabetes better and fight diabetes more effectively on behalf of all people affected by and at risk of diabetes as well as their families and carers.”

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


