{"title":"Comparison of heart failure risk assessment tools among cancer survivors.","authors":"Cheng Hwee Soh, Thomas H Marwick","doi":"10.1186/s40959-024-00267-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cancer survivors have an increased risk of incident heart failure (HF) attributable to shared risk factors and cancer treatment-induced cardiac dysfunction. Selection for HF screening depends on risk assessment, but the optimal means of assessing risk is undefined. We undertook a comparison of HF risk calculators among survivors.</p><p><strong>Methods: </strong>In this study from the UK Biobank, cancer and HF diagnoses were determined based on the International Classification of Diseases (ICD)-10 code and non-cancer participants were included as controls. Participants' risk of incident HF was determined using the Heart Failure Association-International Cardio-oncology Society (HFA-ICOS), the Atherosclerosis Risk in Communities (ARIC-HF) and the Pooled Cohort Equations to Prevent Heart Failure (PCP-HF). The predictive performances of each were compared using the area under the curve (AUC).</p><p><strong>Results: </strong>After propensity matching with age and sex, 9,232 survivors from breast cancer or lymphoma (mean age 59.9 years, 87.8% female), and 23,800 survivors from other cancer types (mean age 59.1 years, 85.8% female) were included in the analysis. The discriminative value for HFA-ICOS (AUC 0.753 [95%CI: 0.739-0.766]) and ARIC-HF (0.757 [95%CI: 0.744-0.770]) were similar, and superior to PCP-HF (0.717 [95%CI: 0.702-0.732]). The overall performance for each risk score was better among participants in other cancer types than those with breast cancer and lymphoma.</p><p><strong>Conclusions: </strong>HFA-ICOS and ARIC-HF outperformed the PCP-HF among cancer- and non-cancer cohort, although all showed modest discrimination for incident HF to be applied to clinical practice. A cancer-specific HF prediction tool could facilitate HF prevention among survivors.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"67"},"PeriodicalIF":3.2000,"publicationDate":"2024-10-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11468191/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00267-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cancer survivors have an increased risk of incident heart failure (HF) attributable to shared risk factors and cancer treatment-induced cardiac dysfunction. Selection for HF screening depends on risk assessment, but the optimal means of assessing risk is undefined. We undertook a comparison of HF risk calculators among survivors.
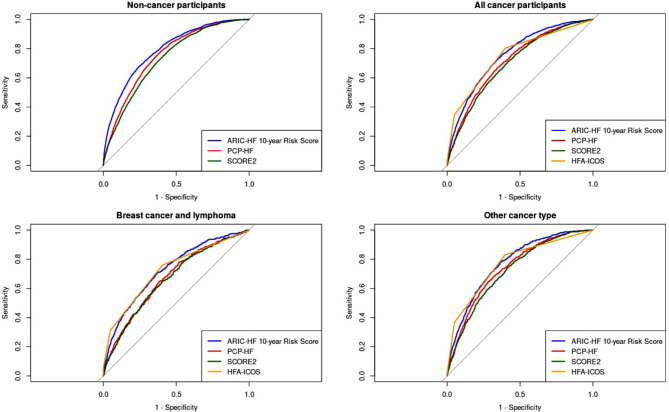
Methods: In this study from the UK Biobank, cancer and HF diagnoses were determined based on the International Classification of Diseases (ICD)-10 code and non-cancer participants were included as controls. Participants' risk of incident HF was determined using the Heart Failure Association-International Cardio-oncology Society (HFA-ICOS), the Atherosclerosis Risk in Communities (ARIC-HF) and the Pooled Cohort Equations to Prevent Heart Failure (PCP-HF). The predictive performances of each were compared using the area under the curve (AUC).
Results: After propensity matching with age and sex, 9,232 survivors from breast cancer or lymphoma (mean age 59.9 years, 87.8% female), and 23,800 survivors from other cancer types (mean age 59.1 years, 85.8% female) were included in the analysis. The discriminative value for HFA-ICOS (AUC 0.753 [95%CI: 0.739-0.766]) and ARIC-HF (0.757 [95%CI: 0.744-0.770]) were similar, and superior to PCP-HF (0.717 [95%CI: 0.702-0.732]). The overall performance for each risk score was better among participants in other cancer types than those with breast cancer and lymphoma.
Conclusions: HFA-ICOS and ARIC-HF outperformed the PCP-HF among cancer- and non-cancer cohort, although all showed modest discrimination for incident HF to be applied to clinical practice. A cancer-specific HF prediction tool could facilitate HF prevention among survivors.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


