Novel Method for Risk Stratification of Major Adverse Clinical Events Using Pre- and Post-Ablation Left Atrial Volume Index in Patients With Persistent Atrial Fibrillation.
{"title":"Novel Method for Risk Stratification of Major Adverse Clinical Events Using Pre- and Post-Ablation Left Atrial Volume Index in Patients With Persistent Atrial Fibrillation.","authors":"Hironori Ishiguchi, Yasuhiro Yoshiga, Akihiko Shimizu, Masakazu Fukuda, Ayumi Omuro, Masahiro Hisaoka, Yusuke Nakashima, Miho Fujita, Shintaro Hashimoto, Takuya Omuro, Toru Ariyoshi, Shigeki Kobayashi, Takayuki Okamura, Motoaki Sano","doi":"10.1253/circrep.CR-24-0062","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The relationship between changes in the left atrial volume index (LAVI) post-catheter ablation (CA) and long-term prognostic events in patients with persistent atrial fibrillation (AF) remains unclear. We evaluated the incidence of major adverse clinical events (MACE), including all-cause death, unplanned heart failure hospitalization, and unplanned cardiovascular hospitalization using pre- and post-CA LAVI.</p><p><strong>Methods and results: </strong>We collected data retrospectively from 150 patients with persistent AF who underwent their first CA. LAVI was calculated during preprocedural echocardiography under AF rhythm (pre-CA LAVI) and 3 months post-CA under sinus rhythm (post-CA LAVI). The cumulative incidence of MACE was compared among 3 subgroups based on the cutoff values of pre-CA (45.5 mL/m<sup>2</sup>) and post-CA (46.5 mL/m<sup>2</sup>; both determined using the c-statistic) LAVI. The subgroup of a pre-CA LAVI >45.5 mL/m<sup>2</sup> with a post-CA LAVI >46.5 mL/m<sup>2</sup> (n=45) had a significantly higher MACE incidence compared with other subgroups (P=0.002). Multivariate analysis identified this subgroup as independently at higher risk for MACE. The subgroup of a pre-CA LAVI >45.5 mL/m<sup>2</sup> with a post-CA LAVI ≤46.5 mL/m<sup>2</sup> (n=49) had an incidence comparable with those with pre-CA LAVI ≤45.5 mL/m<sup>2</sup> (n=56) and exhibited a significantly greater reduction in LAVI than other subgroups did (P<0.001).</p><p><strong>Conclusions: </strong>Combining pre-CA and post-CA LAVIs is valuable in stratifying long-term MACE development risk following CA.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"6 10","pages":"415-423"},"PeriodicalIF":1.1000,"publicationDate":"2024-09-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11464015/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-24-0062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The relationship between changes in the left atrial volume index (LAVI) post-catheter ablation (CA) and long-term prognostic events in patients with persistent atrial fibrillation (AF) remains unclear. We evaluated the incidence of major adverse clinical events (MACE), including all-cause death, unplanned heart failure hospitalization, and unplanned cardiovascular hospitalization using pre- and post-CA LAVI.
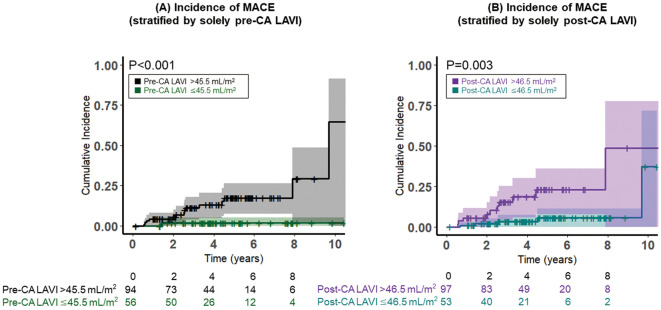
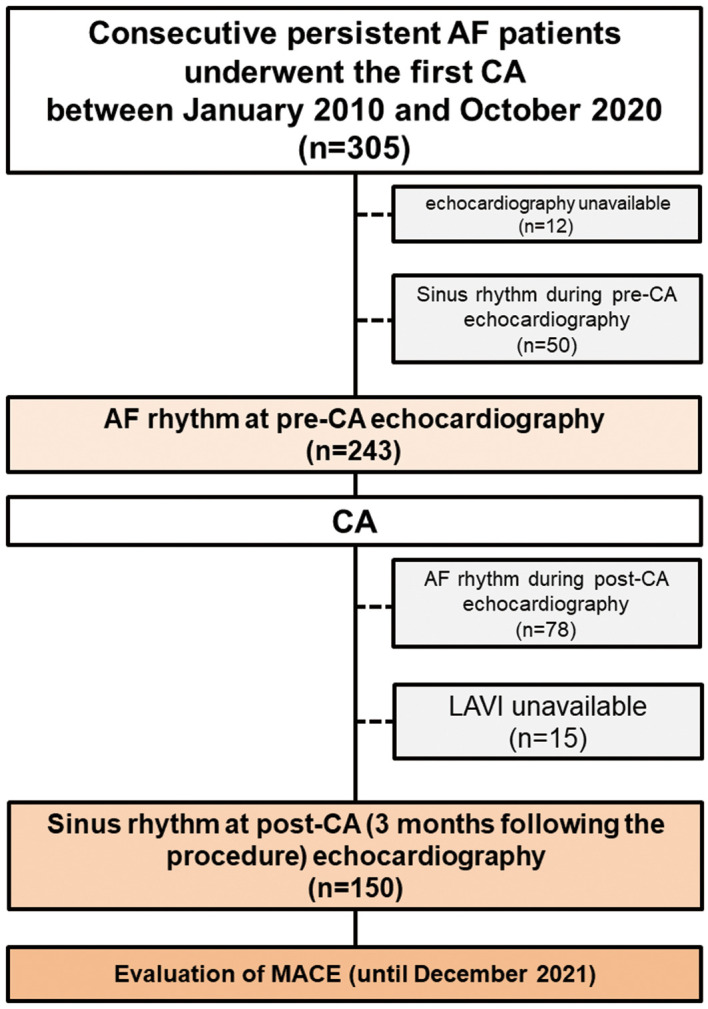
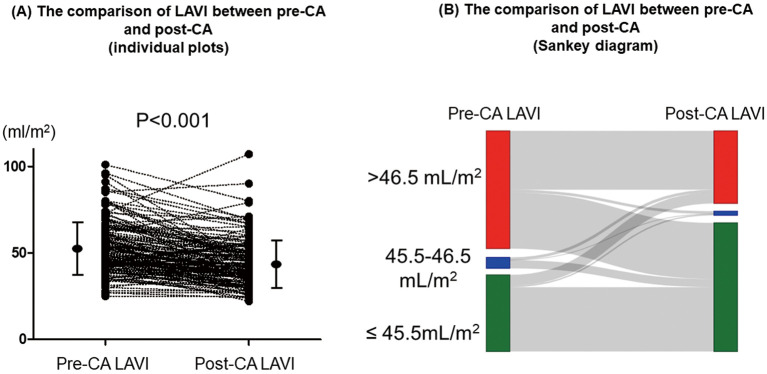
Methods and results: We collected data retrospectively from 150 patients with persistent AF who underwent their first CA. LAVI was calculated during preprocedural echocardiography under AF rhythm (pre-CA LAVI) and 3 months post-CA under sinus rhythm (post-CA LAVI). The cumulative incidence of MACE was compared among 3 subgroups based on the cutoff values of pre-CA (45.5 mL/m2) and post-CA (46.5 mL/m2; both determined using the c-statistic) LAVI. The subgroup of a pre-CA LAVI >45.5 mL/m2 with a post-CA LAVI >46.5 mL/m2 (n=45) had a significantly higher MACE incidence compared with other subgroups (P=0.002). Multivariate analysis identified this subgroup as independently at higher risk for MACE. The subgroup of a pre-CA LAVI >45.5 mL/m2 with a post-CA LAVI ≤46.5 mL/m2 (n=49) had an incidence comparable with those with pre-CA LAVI ≤45.5 mL/m2 (n=56) and exhibited a significantly greater reduction in LAVI than other subgroups did (P<0.001).
Conclusions: Combining pre-CA and post-CA LAVIs is valuable in stratifying long-term MACE development risk following CA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


