Sivasubramanium V. Bhavani, Alexandra Spicer, Pratik Sinha, Albahi Malik, Carlos Lopez-Espina, Lee Schmalz, Gregory L. Watson, Akhil Bhargava, Shah Khan, Dennys Urdiales, Lincoln Updike, Alon Dagan, Hugo Davila, Carmen Demarco, Neil Evans, Falgun Gosai, Karthik Iyer, Niko Kurtzman, Ashok V. Palagiri, Matthew Sims, Scott Smith, Anwaruddin Syed, Deesha Sarma, Bobby Reddy, Philip A. Verhoef, Matthew M. Churpek
{"title":"Distinct immune profiles and clinical outcomes in sepsis subphenotypes based on temperature trajectories","authors":"Sivasubramanium V. Bhavani, Alexandra Spicer, Pratik Sinha, Albahi Malik, Carlos Lopez-Espina, Lee Schmalz, Gregory L. Watson, Akhil Bhargava, Shah Khan, Dennys Urdiales, Lincoln Updike, Alon Dagan, Hugo Davila, Carmen Demarco, Neil Evans, Falgun Gosai, Karthik Iyer, Niko Kurtzman, Ashok V. Palagiri, Matthew Sims, Scott Smith, Anwaruddin Syed, Deesha Sarma, Bobby Reddy, Philip A. Verhoef, Matthew M. Churpek","doi":"10.1007/s00134-024-07669-0","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Purpose</h3><p>Sepsis is a heterogeneous syndrome. Identification of sepsis subphenotypes with distinct immune profiles could lead to targeted therapies. This study investigates the immune profiles of patients with sepsis following distinct body temperature patterns (i.e., temperature trajectory subphenotypes).</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>Hospitalized patients from four hospitals between 2018 and 2022 with suspicion of infection were included. A previously validated temperature trajectory algorithm was used to classify study patients into temperature trajectory subphenotypes. Microbiological profiles, clinical outcomes, and levels of 31 biomarkers were compared between these subphenotypes.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>The 3576 study patients were classified into four temperature trajectory subphenotypes: hyperthermic slow resolvers (<i>N</i> = 563, 16%), hyperthermic fast resolvers (<i>N</i> = 805, 23%), normothermic (<i>N</i> = 1693, 47%), hypothermic (<i>N</i> = 515, 14%). The mortality rate was significantly different between subphenotypes, with the highest rate in hypothermics (14.2%), followed by hyperthermic slow resolvers 6%, normothermic 5.5%, and lowest in hyperthermic fast resolvers 3.6% (<i>p</i> < 0.001). After multiple testing correction for the 31 biomarkers tested, 20 biomarkers remained significantly different between temperature trajectories: angiopoietin-1 (Ang-1), C-reactive protein (CRP), feline McDonough sarcoma-like tyrosine kinase 3 ligand (Flt-3l), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony stimulating factor (GM-CSF), interleukin (IL)-15, IL-1 receptor antagonist (RA), IL-2, IL-6, IL-7, interferon gamma-induced protein 10 (IP-10), monocyte chemoattractant protein-1 (MCP-1), human macrophage inflammatory protein 3 alpha (MIP-3a), neutrophil gelatinase-associated lipocalin (NGAL), pentraxin-3, thrombomodulin, tissue factor, soluble triggering receptor expressed on myeloid cells-1 (sTREM-1), and vascular cellular adhesion molecule-1 (vCAM-1).The hyperthermic fast and slow resolvers had the highest levels of most pro- and anti-inflammatory cytokines. Hypothermics had suppressed levels of most cytokines but the highest levels of several coagulation markers (Ang-1, thrombomodulin, tissue factor).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Sepsis subphenotypes identified using the universally available measurement of body temperature had distinct immune profiles. Hypothermic patients, who had the highest mortality rate, also had the lowest levels of most pro- and anti-inflammatory cytokines.</p>","PeriodicalId":13665,"journal":{"name":"Intensive Care Medicine","volume":"39 1","pages":""},"PeriodicalIF":27.1000,"publicationDate":"2024-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00134-024-07669-0","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
Sepsis is a heterogeneous syndrome. Identification of sepsis subphenotypes with distinct immune profiles could lead to targeted therapies. This study investigates the immune profiles of patients with sepsis following distinct body temperature patterns (i.e., temperature trajectory subphenotypes).
Methods
Hospitalized patients from four hospitals between 2018 and 2022 with suspicion of infection were included. A previously validated temperature trajectory algorithm was used to classify study patients into temperature trajectory subphenotypes. Microbiological profiles, clinical outcomes, and levels of 31 biomarkers were compared between these subphenotypes.
Results
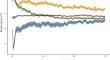
The 3576 study patients were classified into four temperature trajectory subphenotypes: hyperthermic slow resolvers (N = 563, 16%), hyperthermic fast resolvers (N = 805, 23%), normothermic (N = 1693, 47%), hypothermic (N = 515, 14%). The mortality rate was significantly different between subphenotypes, with the highest rate in hypothermics (14.2%), followed by hyperthermic slow resolvers 6%, normothermic 5.5%, and lowest in hyperthermic fast resolvers 3.6% (p < 0.001). After multiple testing correction for the 31 biomarkers tested, 20 biomarkers remained significantly different between temperature trajectories: angiopoietin-1 (Ang-1), C-reactive protein (CRP), feline McDonough sarcoma-like tyrosine kinase 3 ligand (Flt-3l), granulocyte colony stimulating factor (G-CSF), granulocyte-macrophage colony stimulating factor (GM-CSF), interleukin (IL)-15, IL-1 receptor antagonist (RA), IL-2, IL-6, IL-7, interferon gamma-induced protein 10 (IP-10), monocyte chemoattractant protein-1 (MCP-1), human macrophage inflammatory protein 3 alpha (MIP-3a), neutrophil gelatinase-associated lipocalin (NGAL), pentraxin-3, thrombomodulin, tissue factor, soluble triggering receptor expressed on myeloid cells-1 (sTREM-1), and vascular cellular adhesion molecule-1 (vCAM-1).The hyperthermic fast and slow resolvers had the highest levels of most pro- and anti-inflammatory cytokines. Hypothermics had suppressed levels of most cytokines but the highest levels of several coagulation markers (Ang-1, thrombomodulin, tissue factor).
Conclusion
Sepsis subphenotypes identified using the universally available measurement of body temperature had distinct immune profiles. Hypothermic patients, who had the highest mortality rate, also had the lowest levels of most pro- and anti-inflammatory cytokines.
期刊介绍:
Intensive Care Medicine is the premier publication platform fostering the communication and exchange of cutting-edge research and ideas within the field of intensive care medicine on a comprehensive scale. Catering to professionals involved in intensive medical care, including intensivists, medical specialists, nurses, and other healthcare professionals, ICM stands as the official journal of The European Society of Intensive Care Medicine. ICM is dedicated to advancing the understanding and practice of intensive care medicine among professionals in Europe and beyond. The journal provides a robust platform for disseminating current research findings and innovative ideas in intensive care medicine. Content published in Intensive Care Medicine encompasses a wide range, including review articles, original research papers, letters, reviews, debates, and more.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


