{"title":"Autoimmune Hemolytic Anemias: Challenges in Diagnosis and Therapy.","authors":"Wilma Barcellini, Bruno Fattizzo","doi":"10.1159/000540475","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Autoimmune hemolytic anemia (AIHA) is a rare disease due to increased destruction of erythrocytes by autoantibodies, with or without complement activation.</p><p><strong>Summary: </strong>AIHA is usually classified in warm AIHA (wAIHA) and cold agglutinin disease (CAD), based on isotype and thermal amplitude of the autoantibody. The direct antiglobulin test (DAT) or Coombs test is the cornerstone of AIHA diagnosis, as it is positive with anti-IgG in wAIHA, and with anti-C3d/IgM antisera plus high titer cold agglutinins in CAD. Therapy is quite different, as steroids and rituximab are effective in the former, but have a lower response rate and duration in the latter. Splenectomy, which is still a good option for young/fit wAIHA, is contraindicated in CAD, and classic immunosuppressants are moving to further lines. Several new drugs are increasingly used or are in trials for relapsed/refractory AIHAs, including B-cell (parsaclisib, ibrutinib, rilzabrutinib), and plasma cell target therapies (bortezomib, daratumumab), bispecific agents (ianalumab, obexelimab, povetacicept), neonatal Fc receptor blockers (nipocalimab), and complement inhibitors (sutimlimab, riliprubart, pegcetacoplan, iptacopan). Clinically, AIHAs are highly heterogeneous, from mild/compensated to life-threatening/fulminant, and may be primary or associated with infections, neoplasms, autoimmune diseases, transplants, immunodeficiencies, and drugs. Along with all these variables, there are rare forms like mixed (wAIHA plus CAD), atypical (IgA or warm IgM driven), and DAT negative, where the diagnosis and clinical management are particularly challenging.</p><p><strong>Key messages: </strong>This article covers the classic clinical features, diagnosis, and therapy of wAIHA and CAD, and focuses, with the support of clinical vignettes, on difficult diagnosis and refractory/relapsing cases requiring novel therapies.</p>","PeriodicalId":23252,"journal":{"name":"Transfusion Medicine and Hemotherapy","volume":"51 5","pages":"321-331"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11452171/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transfusion Medicine and Hemotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000540475","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Autoimmune hemolytic anemia (AIHA) is a rare disease due to increased destruction of erythrocytes by autoantibodies, with or without complement activation.
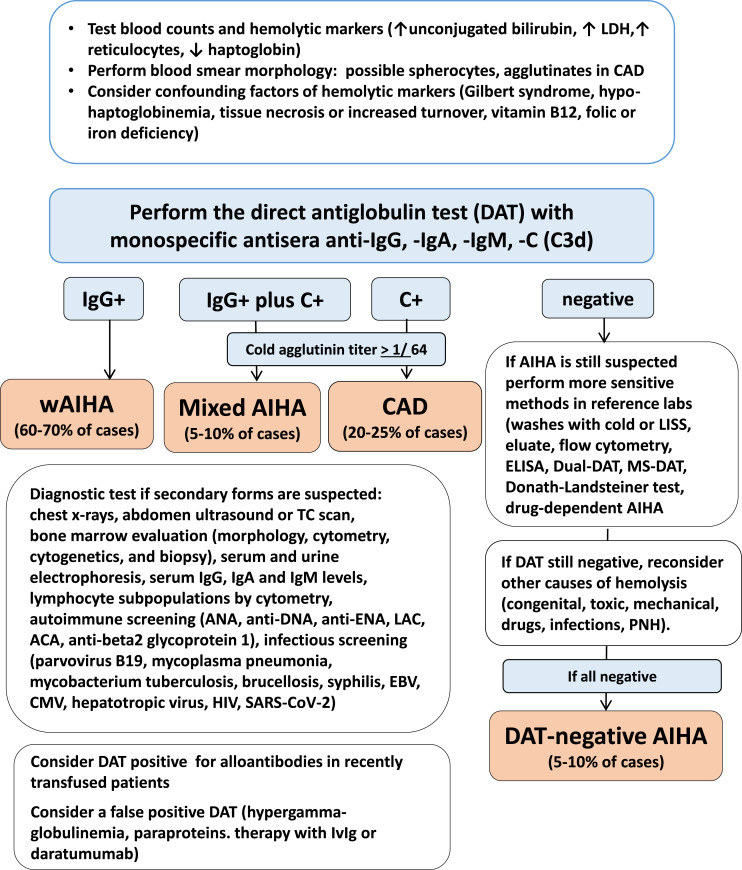
Summary: AIHA is usually classified in warm AIHA (wAIHA) and cold agglutinin disease (CAD), based on isotype and thermal amplitude of the autoantibody. The direct antiglobulin test (DAT) or Coombs test is the cornerstone of AIHA diagnosis, as it is positive with anti-IgG in wAIHA, and with anti-C3d/IgM antisera plus high titer cold agglutinins in CAD. Therapy is quite different, as steroids and rituximab are effective in the former, but have a lower response rate and duration in the latter. Splenectomy, which is still a good option for young/fit wAIHA, is contraindicated in CAD, and classic immunosuppressants are moving to further lines. Several new drugs are increasingly used or are in trials for relapsed/refractory AIHAs, including B-cell (parsaclisib, ibrutinib, rilzabrutinib), and plasma cell target therapies (bortezomib, daratumumab), bispecific agents (ianalumab, obexelimab, povetacicept), neonatal Fc receptor blockers (nipocalimab), and complement inhibitors (sutimlimab, riliprubart, pegcetacoplan, iptacopan). Clinically, AIHAs are highly heterogeneous, from mild/compensated to life-threatening/fulminant, and may be primary or associated with infections, neoplasms, autoimmune diseases, transplants, immunodeficiencies, and drugs. Along with all these variables, there are rare forms like mixed (wAIHA plus CAD), atypical (IgA or warm IgM driven), and DAT negative, where the diagnosis and clinical management are particularly challenging.
Key messages: This article covers the classic clinical features, diagnosis, and therapy of wAIHA and CAD, and focuses, with the support of clinical vignettes, on difficult diagnosis and refractory/relapsing cases requiring novel therapies.
期刊介绍:
This journal is devoted to all areas of transfusion medicine. These include the quality and security of blood products, therapy with blood components and plasma derivatives, transfusion-related questions in transplantation, stem cell manipulation, therapeutic and diagnostic problems of homeostasis, immuno-hematological investigations, and legal aspects of the production of blood products as well as hemotherapy. Both comprehensive reviews and primary publications that detail the newest work in transfusion medicine and hemotherapy promote the international exchange of knowledge within these disciplines. Consistent with this goal, continuing clinical education is also specifically addressed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


