Tatiana Lestido, Kaitlin Ryan-Smith, Alice Werner, Linda Pegram
{"title":"Extreme thrombocytosis negative for GATA1 mutation in an infant with trisomy 21","authors":"Tatiana Lestido, Kaitlin Ryan-Smith, Alice Werner, Linda Pegram","doi":"10.1002/pbc.31352","DOIUrl":null,"url":null,"abstract":"<p>Transient abnormal myelopoiesis (TAM) is characterized by a transient proliferation of abnormal myeloid cells in the bone marrow, leading to an excess of immature cells circulating in the peripheral blood.<span><sup>1</sup></span> TAM diagnosis is associated with the presence of <i>GATA1</i> mutations, but other features such as blasts on peripheral blood smear, flow cytometry immunophenotype, or cytogenetics can be indicative of TAM. This patient's case is unusual due to the <i>GATA1</i> mutation-negative status. The <i>GATA1</i> gene encodes a transcription factor crucial for normal hematopoiesis, and mutations in this gene are associated with myeloid disorders including TAM.<span><sup>2</sup></span> TAM leads to a wide range of hematologic abnormalities and clinical complications, including hyperviscosity syndrome with potential for thrombosis, hydrops fetalis, pericardial effusion, respiratory distress, hypereosinophilia, pseudohyperkalemia, hyperbilirubinemia with liver failure, multiorgan failure, and potential for death.<span><sup>1, 3-5</sup></span> Patients with TAM require timely diagnosis as well as close follow-up, as 20%–30% of these patients subsequently develop myeloid leukemia associated with Down syndrome (ML-DS) before the age of 4 years.<span><sup>6</sup></span> <i>GATA1</i> mutations have, to date, been discovered in nearly all patients with TAM and ML-DS.<span><sup>7</sup></span> The absence of a <i>GATA1</i> mutation in this case raises the question of an alternative molecular mechanism contributing to the development of TAM and extreme thrombocytosis in this patient.</p><p>The patient is a 37-week gestation male delivered via cesarean section due to breech presentation. Birth weight was 2880 g. Promptly upon delivery, the neonate exhibited respiratory compromise necessitating urgent endotracheal intubation and conventional mechanical ventilation.</p><p>He was noted to have distinct facial dysmorphology consistent with trisomy 21. Initial complete blood count (CBC) showed a white blood cell (WBC) count of 25,100/mL with 21% blasts, hemoglobin of 16.7 g/dL, and a platelet count of 633,000/mL.</p><p>While the neonate's oxygen saturation exhibited some improvement following mechanical ventilation, his PaO<sub>2</sub> remained low. A chest x-ray showed no acute cardiopulmonary process. A discrepancy between pre- and post-ductal saturations prompted an echocardiogram, which demonstrated elevated right ventricular pressures, with pulmonary pressures measuring at two-thirds the systemic level, and a patent ductus arteriosus (PDA) characterized by bidirectional flow.</p><p>In light of deteriorating respiratory function and severe pulmonary hypertension, the infant was switched to high-frequency jet ventilation (HFJV). Subsequently, the neonate was transferred to our tertiary care facility. Despite high-frequency jet ventilation, adjunctive inhaled nitric oxide therapy, and administration of corticosteroids at stress dosages, his oxygenation index and clinical condition continued to decline. This downward trajectory necessitated the initiation of veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) on the third day of life, with successful decannulation on the sixth day. This infant required ECMO secondary to his pulmonary hypertension that was not thought to be a consequence of his TAM.</p><p>A CBC on the third day of life revealed a reduction in the WBC count to 16,000/mL with 45% blasts, hemoglobin of 11.4 g/dL, and a platelet count of 252,000/mL.</p><p>Peripheral blood specimen was sent to Hematologics and it was found to have 12% blasts and 1% micromegakaryocytes. Platelets were noted to be increased in number and in size (Figure 1). Flow cytometry confirmed blasts that expressed CD4 and CD36, but lacked CD64 and HLA-DR; an immunophenotype that is associated with myeloid proliferation in patients with Down syndrome.<span><sup>8</sup></span> Sequencing of Exon 2 of <i>GATA1</i> did not find any mutations. Hematologics does not sequence the entire <i>GATA1</i> gene, so next-generation sequencing (NGS) was performed by NEO genomics using their expanded myeloid panel called NeoTYPE Analysis, Myeloid Disorders Profile. No pathogenic mutations were detected in any of the genes, including GATA1, on the NGS panel (Supplemental Figure S1).</p><p>Between Day 3 and Day 15 of life, there was a progressive rise in platelet count, as shown in Table 1. Prophylactic administration of aspirin was started on Day 14 due to a platelet count of greater than two million and the infant's significant risk factor for thrombosis; his carotid end-to-end anastomosis after coming off of ECMO. On Day 13, cytarabine chemotherapy was initiated due to a platelet count of 2,595,000/mL. On the second day of cytarabine therapy, the platelet count peaked at 2,764,000/mL. Patient completed the 7-day course of low-dose cytarabine therapy (1.5 mg/kg/day) on Day 19.<span><sup>9</sup></span> The platelet count declined after completion of the cytarabine course. Beyond the anticipated myelosuppression, the infant did not have any side effects from chemotherapy. The infant has ongoing close follow-up with Hematology/Oncology. He has been clinically well. The platelet count normalized and the WBC count remains normal.</p><p>TAM is a rare hematologic disorder that affects approximately 10%–30% of newborns with trisomy 21.<span><sup>10, 11</sup></span> TAM is characterized by a transient proliferation of abnormal megakaryoblasts and myeloblasts in the bone marrow, leading to an excess of immature cells circulating in the peripheral blood. The underlying molecular mechanism of TAM involves mutations in the <i>GATA1</i> gene, which encodes a transcription factor crucial for normal hematopoiesis. <i>GATA1</i> mutations are detected in most patients with TAM and are considered a hallmark of the disease.<span><sup>12, 13</sup></span> Notably, the neonate in this case was <i>GATA1</i> mutation negative. Despite the absence of a <i>GATA1</i> mutation, the patient's clinical course and laboratory findings strongly supported the diagnosis of TAM. The extreme thrombocytosis with a platelet count that reached 2,764,000/mL of blood is the highest platelet count ever reported in TAM upon our review of the literature.<span><sup>14</sup></span> Low-dose cytarabine resulted in a significant reduction in platelet count after a single cycle. This case presents extreme thrombocytosis in the setting of TAM in a patient without a <i>GATA1</i> mutation, suggesting an alternate molecular pathway contributing to TAM.</p><p>The authors declare no conflicts of interest.</p><p>This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.</p><p>Not required.</p>","PeriodicalId":19822,"journal":{"name":"Pediatric Blood & Cancer","volume":"71 12","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/pbc.31352","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Blood & Cancer","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/pbc.31352","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Transient abnormal myelopoiesis (TAM) is characterized by a transient proliferation of abnormal myeloid cells in the bone marrow, leading to an excess of immature cells circulating in the peripheral blood.1 TAM diagnosis is associated with the presence of GATA1 mutations, but other features such as blasts on peripheral blood smear, flow cytometry immunophenotype, or cytogenetics can be indicative of TAM. This patient's case is unusual due to the GATA1 mutation-negative status. The GATA1 gene encodes a transcription factor crucial for normal hematopoiesis, and mutations in this gene are associated with myeloid disorders including TAM.2 TAM leads to a wide range of hematologic abnormalities and clinical complications, including hyperviscosity syndrome with potential for thrombosis, hydrops fetalis, pericardial effusion, respiratory distress, hypereosinophilia, pseudohyperkalemia, hyperbilirubinemia with liver failure, multiorgan failure, and potential for death.1, 3-5 Patients with TAM require timely diagnosis as well as close follow-up, as 20%–30% of these patients subsequently develop myeloid leukemia associated with Down syndrome (ML-DS) before the age of 4 years.6GATA1 mutations have, to date, been discovered in nearly all patients with TAM and ML-DS.7 The absence of a GATA1 mutation in this case raises the question of an alternative molecular mechanism contributing to the development of TAM and extreme thrombocytosis in this patient.
The patient is a 37-week gestation male delivered via cesarean section due to breech presentation. Birth weight was 2880 g. Promptly upon delivery, the neonate exhibited respiratory compromise necessitating urgent endotracheal intubation and conventional mechanical ventilation.
He was noted to have distinct facial dysmorphology consistent with trisomy 21. Initial complete blood count (CBC) showed a white blood cell (WBC) count of 25,100/mL with 21% blasts, hemoglobin of 16.7 g/dL, and a platelet count of 633,000/mL.
While the neonate's oxygen saturation exhibited some improvement following mechanical ventilation, his PaO2 remained low. A chest x-ray showed no acute cardiopulmonary process. A discrepancy between pre- and post-ductal saturations prompted an echocardiogram, which demonstrated elevated right ventricular pressures, with pulmonary pressures measuring at two-thirds the systemic level, and a patent ductus arteriosus (PDA) characterized by bidirectional flow.
In light of deteriorating respiratory function and severe pulmonary hypertension, the infant was switched to high-frequency jet ventilation (HFJV). Subsequently, the neonate was transferred to our tertiary care facility. Despite high-frequency jet ventilation, adjunctive inhaled nitric oxide therapy, and administration of corticosteroids at stress dosages, his oxygenation index and clinical condition continued to decline. This downward trajectory necessitated the initiation of veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) on the third day of life, with successful decannulation on the sixth day. This infant required ECMO secondary to his pulmonary hypertension that was not thought to be a consequence of his TAM.
A CBC on the third day of life revealed a reduction in the WBC count to 16,000/mL with 45% blasts, hemoglobin of 11.4 g/dL, and a platelet count of 252,000/mL.
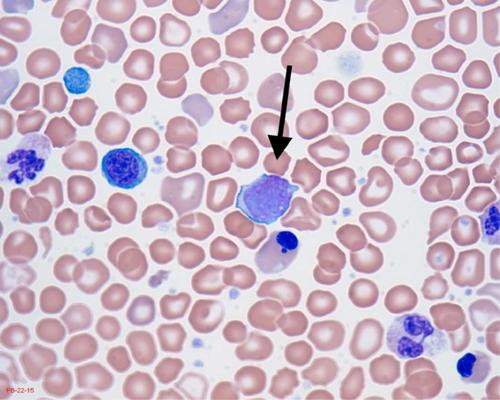
Peripheral blood specimen was sent to Hematologics and it was found to have 12% blasts and 1% micromegakaryocytes. Platelets were noted to be increased in number and in size (Figure 1). Flow cytometry confirmed blasts that expressed CD4 and CD36, but lacked CD64 and HLA-DR; an immunophenotype that is associated with myeloid proliferation in patients with Down syndrome.8 Sequencing of Exon 2 of GATA1 did not find any mutations. Hematologics does not sequence the entire GATA1 gene, so next-generation sequencing (NGS) was performed by NEO genomics using their expanded myeloid panel called NeoTYPE Analysis, Myeloid Disorders Profile. No pathogenic mutations were detected in any of the genes, including GATA1, on the NGS panel (Supplemental Figure S1).
Between Day 3 and Day 15 of life, there was a progressive rise in platelet count, as shown in Table 1. Prophylactic administration of aspirin was started on Day 14 due to a platelet count of greater than two million and the infant's significant risk factor for thrombosis; his carotid end-to-end anastomosis after coming off of ECMO. On Day 13, cytarabine chemotherapy was initiated due to a platelet count of 2,595,000/mL. On the second day of cytarabine therapy, the platelet count peaked at 2,764,000/mL. Patient completed the 7-day course of low-dose cytarabine therapy (1.5 mg/kg/day) on Day 19.9 The platelet count declined after completion of the cytarabine course. Beyond the anticipated myelosuppression, the infant did not have any side effects from chemotherapy. The infant has ongoing close follow-up with Hematology/Oncology. He has been clinically well. The platelet count normalized and the WBC count remains normal.
TAM is a rare hematologic disorder that affects approximately 10%–30% of newborns with trisomy 21.10, 11 TAM is characterized by a transient proliferation of abnormal megakaryoblasts and myeloblasts in the bone marrow, leading to an excess of immature cells circulating in the peripheral blood. The underlying molecular mechanism of TAM involves mutations in the GATA1 gene, which encodes a transcription factor crucial for normal hematopoiesis. GATA1 mutations are detected in most patients with TAM and are considered a hallmark of the disease.12, 13 Notably, the neonate in this case was GATA1 mutation negative. Despite the absence of a GATA1 mutation, the patient's clinical course and laboratory findings strongly supported the diagnosis of TAM. The extreme thrombocytosis with a platelet count that reached 2,764,000/mL of blood is the highest platelet count ever reported in TAM upon our review of the literature.14 Low-dose cytarabine resulted in a significant reduction in platelet count after a single cycle. This case presents extreme thrombocytosis in the setting of TAM in a patient without a GATA1 mutation, suggesting an alternate molecular pathway contributing to TAM.
The authors declare no conflicts of interest.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
血小板计数恢复正常,白细胞计数保持正常。TAM 是一种罕见的血液系统疾病,约有 10%-30% 的新生儿患有 21 三体综合征。10, 11 TAM 的特征是骨髓中异常巨核细胞和髓母细胞的短暂增殖,导致外周血中过量的未成熟细胞循环。TAM 的基本分子机制涉及 GATA1 基因突变,该基因编码一种对正常造血至关重要的转录因子。大多数 TAM 患者都能检测到 GATA1 基因突变,这也是该病的特征之一。尽管没有 GATA1 基因突变,但患者的临床病程和实验室检查结果都有力地支持了 TAM 的诊断。血小板极度增多,血小板计数达到 2,764,000 个/毫升,这是我们查阅文献后发现的 TAM 患者血小板计数最高的病例。本病例显示,在 TAM 的背景下,患者血小板极度减少,但未出现 GATA1 基因突变,这表明导致 TAM 的另一种分子途径。
期刊介绍:
Pediatric Blood & Cancer publishes the highest quality manuscripts describing basic and clinical investigations of blood disorders and malignant diseases of childhood including diagnosis, treatment, epidemiology, etiology, biology, and molecular and clinical genetics of these diseases as they affect children, adolescents, and young adults. Pediatric Blood & Cancer will also include studies on such treatment options as hematopoietic stem cell transplantation, immunology, and gene therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


