Perceived discrimination and refraining from seeking physician's care in Sweden: an intersectional analysis of individual heterogeneity and discriminatory accuracy (AIHDA).
IF 4.1 2区 医学Q1 PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH
Mariam Hassan, Johan Öberg, Maria Wemrell, Raquel Perez Vicente, Martin Lindström, Juan Merlo
{"title":"Perceived discrimination and refraining from seeking physician's care in Sweden: an intersectional analysis of individual heterogeneity and discriminatory accuracy (AIHDA).","authors":"Mariam Hassan, Johan Öberg, Maria Wemrell, Raquel Perez Vicente, Martin Lindström, Juan Merlo","doi":"10.1186/s12939-024-02291-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Discrimination may further impede access to medical care for individuals in socially disadvantaged positions. Sociodemographic information and perceived discrimination intersect and define multiple contexts or strata that condition the risk of refraining from seeking physician's care. By applying analysis of individual heterogeneity and discriminatory accuracy (AIHDA) we aimed to improve the mapping of risk by considering both strata average risk differences and the accuracy of such strata risks for distinguishing between individuals who did or did not refrain from seeking physician's care.</p><p><strong>Methods: </strong>We analysed nine annual National Public Health Surveys (2004, 2007-2014) in Sweden including 73,815 participants. We investigated the risk of refraining from seeking physician's care across 64 intersectional strata defined by sex, education, age, country of birth, and perceived discrimination. We calculated strata-specific prevalences and prevalence ratios (PR) with 95% confidence intervals (CI), and the area under the receiver operating characteristic curve (AUC) to evaluate the discriminatory accuracy (DA).</p><p><strong>Results: </strong>Discriminated foreign-born women aged 35-49 with a low educational level show a six times higher risk (PR = 6.07, 95% CI 5.05-7.30) than non-discriminated native men with a high educational level aged 35-49. However, the DA of the intersectional strata was small (AUC = 0.64). Overall, discrimination increased the absolute risk of refraining from seeking physician's care, over and above age, sex, and educational level.</p><p><strong>Conclusions: </strong>AIHDA disclosed complex intersectional inequalities in the average risk of refraining from seeking physician's care. This risk was rather high in some strata, which is relevant from an individual perspective. However, from a population perspective, the low DA of the intersectional strata suggests that potential interventions to reduce such inequalities should be universal but tailored to the specific contextual characteristics of the strata. Discrimination impairs access to healthcare.</p>","PeriodicalId":13745,"journal":{"name":"International Journal for Equity in Health","volume":"23 1","pages":"199"},"PeriodicalIF":4.1000,"publicationDate":"2024-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11452949/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal for Equity in Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12939-024-02291-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Discrimination may further impede access to medical care for individuals in socially disadvantaged positions. Sociodemographic information and perceived discrimination intersect and define multiple contexts or strata that condition the risk of refraining from seeking physician's care. By applying analysis of individual heterogeneity and discriminatory accuracy (AIHDA) we aimed to improve the mapping of risk by considering both strata average risk differences and the accuracy of such strata risks for distinguishing between individuals who did or did not refrain from seeking physician's care.
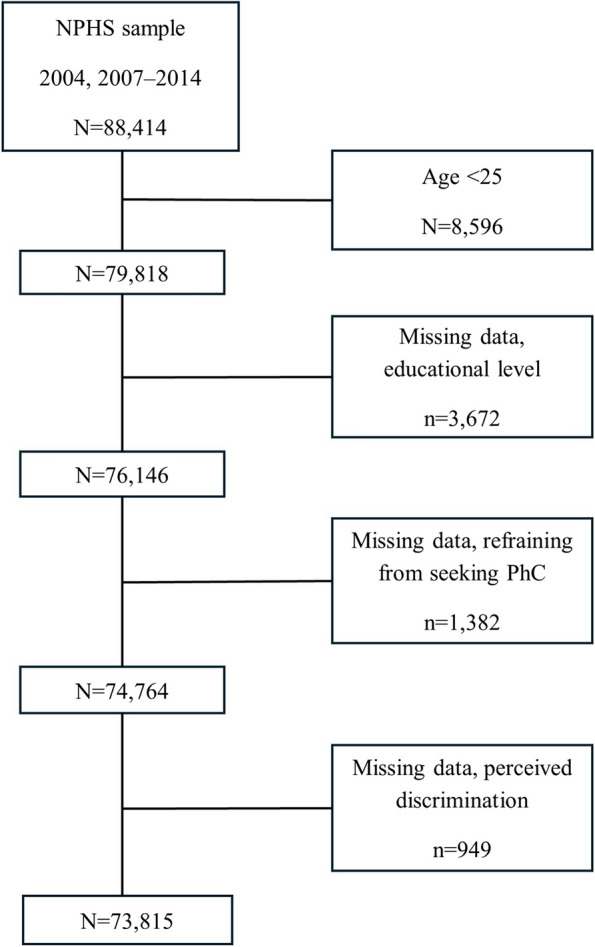
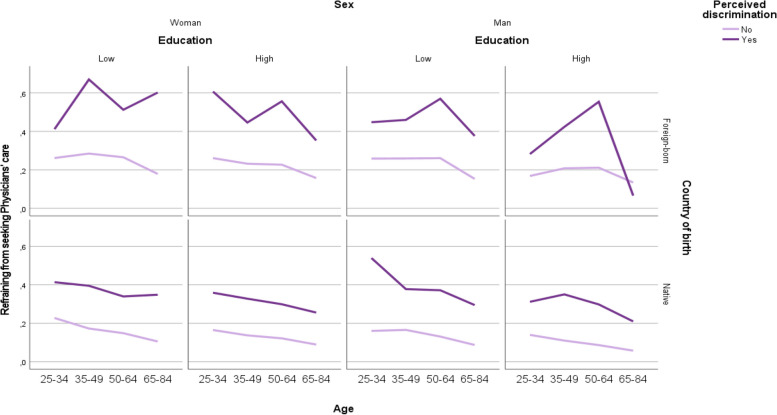
Methods: We analysed nine annual National Public Health Surveys (2004, 2007-2014) in Sweden including 73,815 participants. We investigated the risk of refraining from seeking physician's care across 64 intersectional strata defined by sex, education, age, country of birth, and perceived discrimination. We calculated strata-specific prevalences and prevalence ratios (PR) with 95% confidence intervals (CI), and the area under the receiver operating characteristic curve (AUC) to evaluate the discriminatory accuracy (DA).
Results: Discriminated foreign-born women aged 35-49 with a low educational level show a six times higher risk (PR = 6.07, 95% CI 5.05-7.30) than non-discriminated native men with a high educational level aged 35-49. However, the DA of the intersectional strata was small (AUC = 0.64). Overall, discrimination increased the absolute risk of refraining from seeking physician's care, over and above age, sex, and educational level.
Conclusions: AIHDA disclosed complex intersectional inequalities in the average risk of refraining from seeking physician's care. This risk was rather high in some strata, which is relevant from an individual perspective. However, from a population perspective, the low DA of the intersectional strata suggests that potential interventions to reduce such inequalities should be universal but tailored to the specific contextual characteristics of the strata. Discrimination impairs access to healthcare.
期刊介绍:
International Journal for Equity in Health is an Open Access, peer-reviewed, online journal presenting evidence relevant to the search for, and attainment of, equity in health across and within countries. International Journal for Equity in Health aims to improve the understanding of issues that influence the health of populations. This includes the discussion of political, policy-related, economic, social and health services-related influences, particularly with regard to systematic differences in distributions of one or more aspects of health in population groups defined demographically, geographically, or socially.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


