{"title":"Intrabiliary pressure in the pathophysiology of extra hepatic biliary obstruction.","authors":"Dhananjay Saxena, Shridhar Vasantrao Sasturkar, Amar Mukund, Yashwant Patidar, Ashok Kumar Choudhury, Ragini Kilambi, Pratibha Kale","doi":"10.14744/hf.2023.2023.0066","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aim: </strong>The aim of this study was to evaluate the role of intrabiliary pressure (IBP) in the pathophysiology of extrahepatic biliary obstruction (EHBO) during percutaneous transhepatic biliary drainage (PTBD).</p><p><strong>Materials and methods: </strong>Adult patients with EHBO who underwent PTBD were prospectively enrolled. IBP was recorded during primary PTBD. The parameters of interest were age, gender, etiology of EHBO, baseline and post-PTBD liver function tests, duration for resolution of jaundice (decrease in total serum bilirubin ≥30% of baseline or <2 mg/dL), cholangitis, bile cultures, and serum albumin levels. The level of EHBO was divided into three types: Type 1 - secondary biliary confluence involved; Type 2 - primary biliary confluence involved; Type 3 - mid and distal common bile duct obstruction.</p><p><strong>Results: </strong>IBP was measured in 102 patients, and finally, 87 patients, including 52 (59.77%) females, were analyzed. The mean age of the patients was 56.1±11.6 years. The most common etiology of EHBO was carcinoma of the gallbladder in 44 (50.6%) patients. The mean IBP was 18.41±3.91 mmHg. IBP was significantly higher in Type 3 EHBO compared to Type 1 and 2 (p=0.012). A significant correlation was seen between IBP and baseline total serum bilirubin (p<0.01). There was a negative correlation between IBP and baseline serum albumin (p=0.017). In 56.3% of patients, resolution of jaundice was observed by day 3, but this was not significantly associated with IBP (p=0.19). There was no correlation between IBP and cholangitis (p=0.97) or bacterial cultures (p=0.21).</p><p><strong>Conclusion: </strong>IBP was significantly associated with the type of EHBO, baseline serum bilirubin, and albumin levels. IBP could not predict cholangitis or the resolution of jaundice after PTBD.</p>","PeriodicalId":29722,"journal":{"name":"Hepatology Forum","volume":"5 4","pages":"198-203"},"PeriodicalIF":2.1000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11440221/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/hf.2023.2023.0066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aim: The aim of this study was to evaluate the role of intrabiliary pressure (IBP) in the pathophysiology of extrahepatic biliary obstruction (EHBO) during percutaneous transhepatic biliary drainage (PTBD).
Materials and methods: Adult patients with EHBO who underwent PTBD were prospectively enrolled. IBP was recorded during primary PTBD. The parameters of interest were age, gender, etiology of EHBO, baseline and post-PTBD liver function tests, duration for resolution of jaundice (decrease in total serum bilirubin ≥30% of baseline or <2 mg/dL), cholangitis, bile cultures, and serum albumin levels. The level of EHBO was divided into three types: Type 1 - secondary biliary confluence involved; Type 2 - primary biliary confluence involved; Type 3 - mid and distal common bile duct obstruction.
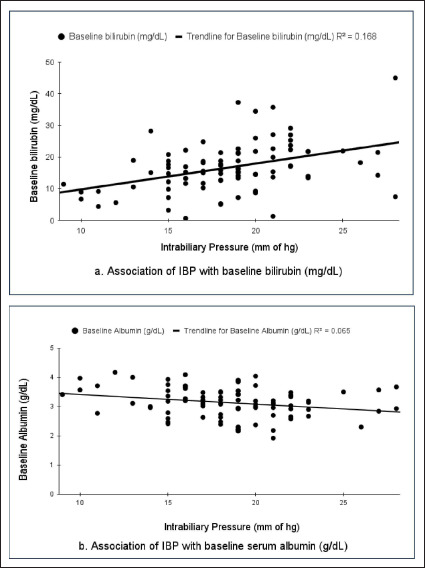
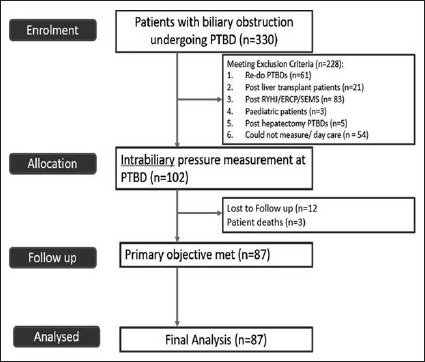
Results: IBP was measured in 102 patients, and finally, 87 patients, including 52 (59.77%) females, were analyzed. The mean age of the patients was 56.1±11.6 years. The most common etiology of EHBO was carcinoma of the gallbladder in 44 (50.6%) patients. The mean IBP was 18.41±3.91 mmHg. IBP was significantly higher in Type 3 EHBO compared to Type 1 and 2 (p=0.012). A significant correlation was seen between IBP and baseline total serum bilirubin (p<0.01). There was a negative correlation between IBP and baseline serum albumin (p=0.017). In 56.3% of patients, resolution of jaundice was observed by day 3, but this was not significantly associated with IBP (p=0.19). There was no correlation between IBP and cholangitis (p=0.97) or bacterial cultures (p=0.21).
Conclusion: IBP was significantly associated with the type of EHBO, baseline serum bilirubin, and albumin levels. IBP could not predict cholangitis or the resolution of jaundice after PTBD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


