One-Year Prognosis Difference of Myocardial Infarction With or Without Coronary Obstruction in Developing Countries: Insights From the Moroccan Experience.
Amine Bouchlarhem, Ihssane Merimi, Zakaria Bazid, Nabila Ismaili, Noha El Ouafi
{"title":"One-Year Prognosis Difference of Myocardial Infarction With or Without Coronary Obstruction in Developing Countries: Insights From the Moroccan Experience.","authors":"Amine Bouchlarhem, Ihssane Merimi, Zakaria Bazid, Nabila Ismaili, Noha El Ouafi","doi":"10.1177/11795468241282855","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The debate remains open as to the difference in prevalence of mortality and occurrence of acute events in patients with Myocardial infarction with non-obstructive coronary arteries (MINOCA) and others with Myocardial infarction with coronary arteries disease (MI-CAD).</p><p><strong>Methods: </strong>We conducted a 2-year retrospective study for patients admitted for Acute coronary syndrome (ACS) to analyze the clinical and prognostic characteristics of patients with MINOCA versus MI-CAD. We defined 1-year all-cause mortality as the primary outcome, and the secondary outcome as a composite of 1-year readmission for myocardial infarction or acute heart failure (AHF).</p><p><strong>Results: </strong>Our study included 1077 patients, 95.3% with MI-CAD and 4.7% with MINOCA. At admission, 71.1% patient were diagnosed STEMI and 28.9% with NSTEMI. The difference between the 2 groups was found on age (<i>P</i> < .001), hypertension, diabetes with consecutive <i>P</i>-values of .007 and .001, as well as Ejection fraction (<i>P</i> < .001). For the outcomes studied, the difference was significant between the 2 groups for all events, and MINOCA patients had a better prognosis than MI-CAD patients, with adjusted hazard ratios (HR) for 1-year mortality (HR = 0.601 <i>P</i> = .004), for readmission for ACS (HR = 0.662; <i>P</i> = .002) and for readmission for AHF (HR = 0.539; <i>P</i> = .019).</p><p><strong>Conclusion: </strong>Despite the ambiguity in the genesis of MINOCA, the short- and long-term prognosis of these patients remains generally favorable.</p>","PeriodicalId":10419,"journal":{"name":"Clinical Medicine Insights. Cardiology","volume":"18 ","pages":"11795468241282855"},"PeriodicalIF":3.3000,"publicationDate":"2024-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11440553/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795468241282855","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The debate remains open as to the difference in prevalence of mortality and occurrence of acute events in patients with Myocardial infarction with non-obstructive coronary arteries (MINOCA) and others with Myocardial infarction with coronary arteries disease (MI-CAD).
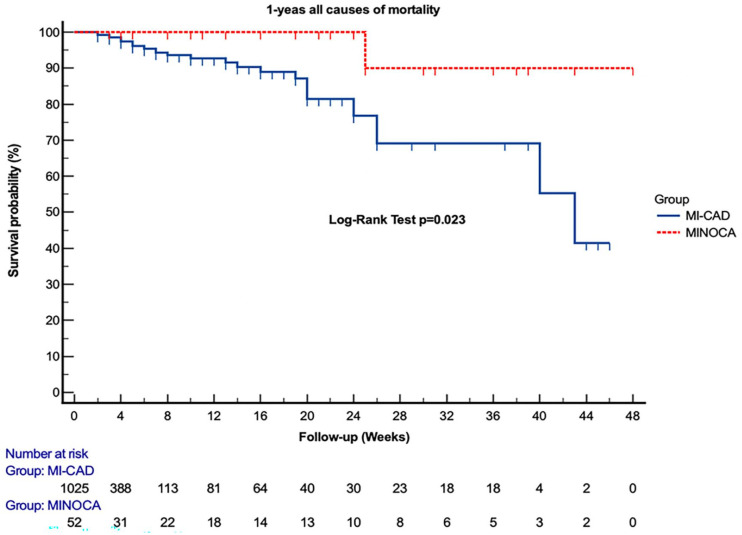
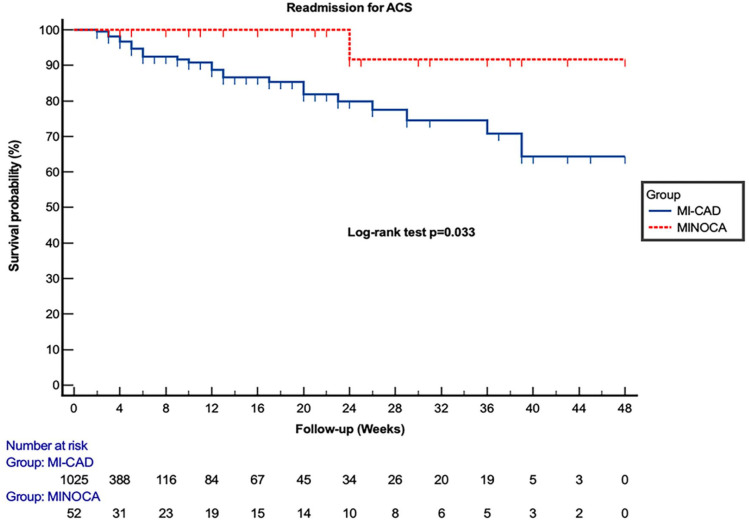
Methods: We conducted a 2-year retrospective study for patients admitted for Acute coronary syndrome (ACS) to analyze the clinical and prognostic characteristics of patients with MINOCA versus MI-CAD. We defined 1-year all-cause mortality as the primary outcome, and the secondary outcome as a composite of 1-year readmission for myocardial infarction or acute heart failure (AHF).
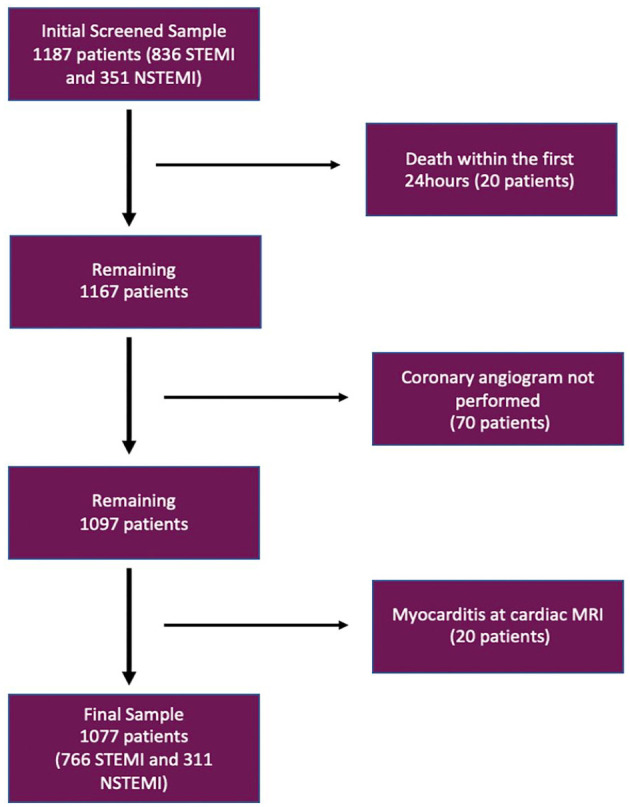
Results: Our study included 1077 patients, 95.3% with MI-CAD and 4.7% with MINOCA. At admission, 71.1% patient were diagnosed STEMI and 28.9% with NSTEMI. The difference between the 2 groups was found on age (P < .001), hypertension, diabetes with consecutive P-values of .007 and .001, as well as Ejection fraction (P < .001). For the outcomes studied, the difference was significant between the 2 groups for all events, and MINOCA patients had a better prognosis than MI-CAD patients, with adjusted hazard ratios (HR) for 1-year mortality (HR = 0.601 P = .004), for readmission for ACS (HR = 0.662; P = .002) and for readmission for AHF (HR = 0.539; P = .019).
Conclusion: Despite the ambiguity in the genesis of MINOCA, the short- and long-term prognosis of these patients remains generally favorable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


