{"title":"Death and taxes: Lactate and the Laffer curve","authors":"Rose D. Nolen-Walston, Michael J. Mandel","doi":"10.1111/vcp.13387","DOIUrl":null,"url":null,"abstract":"<p>In 1980, Ronald Reagan was elected as a president on a simple platform: the need for tax cuts to revive the economy, which was struggling at the time. His theory, and the theory of the supply-side economists who supported him, was simple. Business owners are more likely to hire new workers and invest in new equipment if their after-tax income goes up. The supply-siders of the day believed that if federal tax rates were cut, especially at the top end, business owners would expand, boosting both employment and investment, increasing growth, and potentially even reducing inflation, which was a big problem at the time. Thus, the benefits of the tax cut would “trickle down” to all Americans. One of the main proponents of this theory was an economist called Arthur Laffer, who, in 1974, had been enjoying a late-night supper with a few Republican policy wonks (including Dick Cheney and Donald Rumsfeld, as it happened). The topic of conversation was tax rate and government income and whether President Ford's tax hikes would spur increases in federal revenue. Not necessarily, suggested Laffer, who reportedly whipped out a pen and made the following sketch on his napkin (Figure 1).<span><sup>1</sup></span>\n </p><p>On the x-axis, we see tax rates ranging from 0% to 100%, and on the y-axis, there is government revenue. It is clear that a tax rate of 0% results in zero income, and the coffers are dry. Conversely, though, Laffer pointed out that a tax rate of 100% would result in the same thing. If the government takes every cent of your salary, you are clearly not going to work at all. So, what if, suggests Laffer's curve, we are here, point A in Figure 2, on the tax curve?</p><p>In this case, high tax rates are actually suppressing taxpayer's capitalist urges. A reduction in the tax rate to point B will paradoxically result in an increase in revenue, not a decrease, as shown here in Figure 3.</p><p>This was an odd thought. Could a drop in the tax rate really increase the amount of money the government collected? We avoid political commentary and allow readers their own interpretation of history as to the results of this experiment.<span><sup>2</sup></span> However, this concept has an interesting application in the consideration of physiology.</p><p>Take lactate, for example. L-lactate is produced by the mammalian cell as a product of anaerobic metabolism,<span><sup>3</sup></span> and is often used clinically as a measure of tissue perfusion. Blood lactate concentration not only assesses both the rate of production as well as clearance,<span><sup>4</sup></span> but also, in the very end, it is limited by the capacity of the heart and peripheral vasculature to mobilize the tissue-produced lactate and carry venous blood back to the sampling point. As such, lactate acts as the scorecard of the body; though blood lactate levels cannot tell you what is wrong or how to fix it, it provides useful information to clinicians as to whether they are winning the battle… or losing it.<span><sup>5-7</sup></span>\n </p><p>But perhaps it is a little more complicated than that? Applying Laffer's curve to lactate kinetics, our schematic in Figure 4 assigns an overall value for perfusion (or oxygen delivery) on the x-axis, but with the values flip-flopped from the original graph shown above. On the left is 100%, suggesting perfect perfusion, and 0% on the right, showing a cessation of circulatory function, commonly described as death. As tissue perfusion drops globally, blood lactate concentrations begin to climb from a baseline of around 1 mmol/L.</p><p>However, as systemic disease results in hypoperfusion or mitochondrial injury, oxygen delivery and extraction fall, causing organ dysfunction at the cellular and subcellular level. Anaerobic metabolism prevails, and L-lactate production increases rapidly. Increased glycolysis, inhibition of pyruvate dehydrogenase, and reduced hepatic utilization may further add to the accumulation of lactate in the blood.<span><sup>8</sup></span> Toward the terminal stage of this process, as cardiac output plummets, lactate produced in peripheral tissues is presumably no longer mobilized but simply accumulates in situ, and blood concentration may no longer reflect tissue levels. At the point when perfusion ceases entirely, anaerobic metabolism fails, too, and lactate production drops to zero. In that case, the final segment of the blood lactate curve might look like Figure 5.</p><p>What is the relevance of this to the clinician? Imagine a patient whose blood lactate is 4 mmol/L, as in Figure 6. The vast majority of patients with blood lactate values around this number will be on the left-hand side of the curve: moderately compromised, but not drastically so. They meet the standard cutoff for shock,<span><sup>9</sup></span> but only just.</p><p>Occasionally, though, we see a patient whose lactate level does not fit their clinical picture. Though the measured L-lactate is still 4 mmol/L, they seem much sicker than that predicted by our clinical gestalt. They are cold and nonresponsive, their heart rate is surprisingly higher or lower than we might expect, and the severity of hypotension suggests impending circulatory collapse. Is this just a fluke of biology, or is there an explanation for these cases? It may be that a small percentage of these patients have lactate values that reflect the right-hand side of the curve, as shown here in Figure 7.</p><p>Perhaps these are the patients whose lactate seems inexplicably too low for their clinical presentation. They might even show a transient increase in blood lactate as resuscitation progresses, their perfusion improves, and their lactate values backtrack along the curve. They could comprise some of the cases that skeptics point at when they argue that lactate is not a specific predictor of outcome, as many of them die even with vigorous treatment despite a comparatively modest lactate level. If, as Arthur Laffer has noted, “There are always two tax rates that yield the same revenues,”<span><sup>1</sup></span> then perhaps there are two states of perfusion that return the same blood lactate concentrations? Though it is still debated whether Reagan's Tax Act of 1981 followed Laffer's curve by increasing revenue while lowering taxes,<span><sup>2</sup></span> his spontaneous cartoon may still be useful in offering a graphical explanation of a simple but interesting thought experiment in critical care medicine.</p><p>No conflict of interest is declared.</p>","PeriodicalId":23593,"journal":{"name":"Veterinary clinical pathology","volume":"53 3","pages":"291-293"},"PeriodicalIF":1.1000,"publicationDate":"2024-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/vcp.13387","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Veterinary clinical pathology","FirstCategoryId":"97","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/vcp.13387","RegionNum":4,"RegionCategory":"农林科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
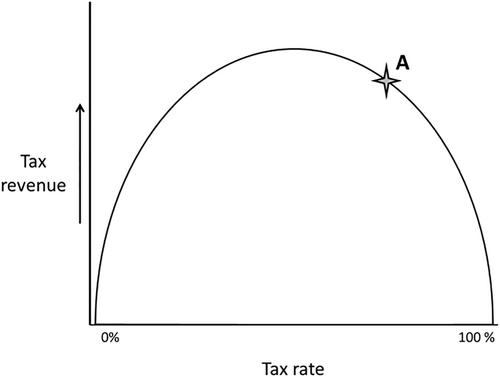
In 1980, Ronald Reagan was elected as a president on a simple platform: the need for tax cuts to revive the economy, which was struggling at the time. His theory, and the theory of the supply-side economists who supported him, was simple. Business owners are more likely to hire new workers and invest in new equipment if their after-tax income goes up. The supply-siders of the day believed that if federal tax rates were cut, especially at the top end, business owners would expand, boosting both employment and investment, increasing growth, and potentially even reducing inflation, which was a big problem at the time. Thus, the benefits of the tax cut would “trickle down” to all Americans. One of the main proponents of this theory was an economist called Arthur Laffer, who, in 1974, had been enjoying a late-night supper with a few Republican policy wonks (including Dick Cheney and Donald Rumsfeld, as it happened). The topic of conversation was tax rate and government income and whether President Ford's tax hikes would spur increases in federal revenue. Not necessarily, suggested Laffer, who reportedly whipped out a pen and made the following sketch on his napkin (Figure 1).1
On the x-axis, we see tax rates ranging from 0% to 100%, and on the y-axis, there is government revenue. It is clear that a tax rate of 0% results in zero income, and the coffers are dry. Conversely, though, Laffer pointed out that a tax rate of 100% would result in the same thing. If the government takes every cent of your salary, you are clearly not going to work at all. So, what if, suggests Laffer's curve, we are here, point A in Figure 2, on the tax curve?
In this case, high tax rates are actually suppressing taxpayer's capitalist urges. A reduction in the tax rate to point B will paradoxically result in an increase in revenue, not a decrease, as shown here in Figure 3.
This was an odd thought. Could a drop in the tax rate really increase the amount of money the government collected? We avoid political commentary and allow readers their own interpretation of history as to the results of this experiment.2 However, this concept has an interesting application in the consideration of physiology.
Take lactate, for example. L-lactate is produced by the mammalian cell as a product of anaerobic metabolism,3 and is often used clinically as a measure of tissue perfusion. Blood lactate concentration not only assesses both the rate of production as well as clearance,4 but also, in the very end, it is limited by the capacity of the heart and peripheral vasculature to mobilize the tissue-produced lactate and carry venous blood back to the sampling point. As such, lactate acts as the scorecard of the body; though blood lactate levels cannot tell you what is wrong or how to fix it, it provides useful information to clinicians as to whether they are winning the battle… or losing it.5-7
But perhaps it is a little more complicated than that? Applying Laffer's curve to lactate kinetics, our schematic in Figure 4 assigns an overall value for perfusion (or oxygen delivery) on the x-axis, but with the values flip-flopped from the original graph shown above. On the left is 100%, suggesting perfect perfusion, and 0% on the right, showing a cessation of circulatory function, commonly described as death. As tissue perfusion drops globally, blood lactate concentrations begin to climb from a baseline of around 1 mmol/L.
However, as systemic disease results in hypoperfusion or mitochondrial injury, oxygen delivery and extraction fall, causing organ dysfunction at the cellular and subcellular level. Anaerobic metabolism prevails, and L-lactate production increases rapidly. Increased glycolysis, inhibition of pyruvate dehydrogenase, and reduced hepatic utilization may further add to the accumulation of lactate in the blood.8 Toward the terminal stage of this process, as cardiac output plummets, lactate produced in peripheral tissues is presumably no longer mobilized but simply accumulates in situ, and blood concentration may no longer reflect tissue levels. At the point when perfusion ceases entirely, anaerobic metabolism fails, too, and lactate production drops to zero. In that case, the final segment of the blood lactate curve might look like Figure 5.
What is the relevance of this to the clinician? Imagine a patient whose blood lactate is 4 mmol/L, as in Figure 6. The vast majority of patients with blood lactate values around this number will be on the left-hand side of the curve: moderately compromised, but not drastically so. They meet the standard cutoff for shock,9 but only just.
Occasionally, though, we see a patient whose lactate level does not fit their clinical picture. Though the measured L-lactate is still 4 mmol/L, they seem much sicker than that predicted by our clinical gestalt. They are cold and nonresponsive, their heart rate is surprisingly higher or lower than we might expect, and the severity of hypotension suggests impending circulatory collapse. Is this just a fluke of biology, or is there an explanation for these cases? It may be that a small percentage of these patients have lactate values that reflect the right-hand side of the curve, as shown here in Figure 7.
Perhaps these are the patients whose lactate seems inexplicably too low for their clinical presentation. They might even show a transient increase in blood lactate as resuscitation progresses, their perfusion improves, and their lactate values backtrack along the curve. They could comprise some of the cases that skeptics point at when they argue that lactate is not a specific predictor of outcome, as many of them die even with vigorous treatment despite a comparatively modest lactate level. If, as Arthur Laffer has noted, “There are always two tax rates that yield the same revenues,”1 then perhaps there are two states of perfusion that return the same blood lactate concentrations? Though it is still debated whether Reagan's Tax Act of 1981 followed Laffer's curve by increasing revenue while lowering taxes,2 his spontaneous cartoon may still be useful in offering a graphical explanation of a simple but interesting thought experiment in critical care medicine.
期刊介绍:
Veterinary Clinical Pathology is the official journal of the American Society for Veterinary Clinical Pathology (ASVCP) and the European Society of Veterinary Clinical Pathology (ESVCP). The journal''s mission is to provide an international forum for communication and discussion of scientific investigations and new developments that advance the art and science of laboratory diagnosis in animals. Veterinary Clinical Pathology welcomes original experimental research and clinical contributions involving domestic, laboratory, avian, and wildlife species in the areas of hematology, hemostasis, immunopathology, clinical chemistry, cytopathology, surgical pathology, toxicology, endocrinology, laboratory and analytical techniques, instrumentation, quality assurance, and clinical pathology education.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


