Shuaib Hafid, Sarina R Isenberg, Aleisha Fernandes, Erin Gallagher, Colleen Webber, Meera Joseph, Manish M Sood, Adrianna Bruni, Janet L Davis, Grace Warmels, James Downar, Anastasia Gayowsky, Aaron Jones, Doug Manuel, Peter Tanuseputro, Michelle Howard
{"title":"End-of-Life Care Among Patients With Kidney Failure on Maintenance Dialysis: A Retrospective Population-Based Study.","authors":"Shuaib Hafid, Sarina R Isenberg, Aleisha Fernandes, Erin Gallagher, Colleen Webber, Meera Joseph, Manish M Sood, Adrianna Bruni, Janet L Davis, Grace Warmels, James Downar, Anastasia Gayowsky, Aaron Jones, Doug Manuel, Peter Tanuseputro, Michelle Howard","doi":"10.1177/20543581241280698","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nephrologists routinely provide end-of-life care for patients with kidney failure (KF) on maintenance dialysis. Involvement of primary care and palliative care physicians may enhance this experience.</p><p><strong>Objective: </strong>The objective was to describe outpatient care patterns in the last year of life and the end-of-life acute care utilization for patients with KF on maintenance dialysis.</p><p><strong>Design: </strong>Retrospective cohort study using population-level health administrative data.</p><p><strong>Setting & participants: </strong>Outpatient and inpatient care during the last year of life among patients who died between 2017 and 2019, receiving maintenance dialysis in Ontario, Canada.</p><p><strong>Measurements: </strong>The primary exposure is patterns of physician specialties providing outpatient care in the last year of life. Outcomes include outpatient encounters in the last year of life, acute care visitation in the last month of life, and place of death.</p><p><strong>Methods: </strong>We reported the count and percentage of categorical outcomes and the median (interquartile range) for numeric outcomes. We produced time series plots of the mean monthly percentage of encounters to different specialties stratified by physician specialty patterns. We evaluated differences in outcomes by physician specialty patterns using analysis of variance (ANOVA) and Pearson's chi-square tests (<i>P</i> < .05, two-tailed).</p><p><strong>Results: </strong>Among 6866 patients, the median age at death was 73, 36.1% were female, and 87.8% resided in urban regions. Three patterns emerged: a primary care, nephrology, and palliative care triad (25.5%); a primary care and nephrology dyad (59.3%); and a non-primary care pattern (15.2%). Palliative care involvement is concentrated near death. Of all, 81.4% spent at least 1 day in hospital or emergency department in the last month, but those with primary care, palliative care, and nephrology involvement had the fewest acute care deaths (65.8%).</p><p><strong>Limitations: </strong>Outpatient care patterns were defined using physician billing codes, potentially missing care from other providers.</p><p><strong>Conclusions: </strong>Nephrology and primary care predominantly manage outpatient care in the last year of life for patients with KF on maintenance dialysis, with consistent acute care use across care patterns except for the place of death. Future research should explore associations between patterns of care and end-of-life outcomes to identify the most optimal model of care for patients with KF on maintenance dialysis.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241280698"},"PeriodicalIF":1.5000,"publicationDate":"2024-09-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11418337/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241280698","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Nephrologists routinely provide end-of-life care for patients with kidney failure (KF) on maintenance dialysis. Involvement of primary care and palliative care physicians may enhance this experience.
Objective: The objective was to describe outpatient care patterns in the last year of life and the end-of-life acute care utilization for patients with KF on maintenance dialysis.
Design: Retrospective cohort study using population-level health administrative data.
Setting & participants: Outpatient and inpatient care during the last year of life among patients who died between 2017 and 2019, receiving maintenance dialysis in Ontario, Canada.
Measurements: The primary exposure is patterns of physician specialties providing outpatient care in the last year of life. Outcomes include outpatient encounters in the last year of life, acute care visitation in the last month of life, and place of death.
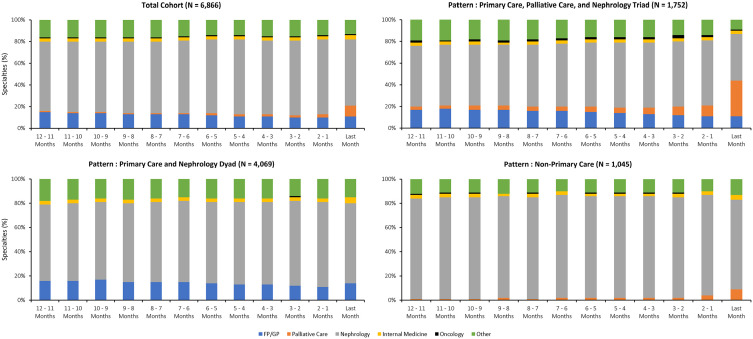
Methods: We reported the count and percentage of categorical outcomes and the median (interquartile range) for numeric outcomes. We produced time series plots of the mean monthly percentage of encounters to different specialties stratified by physician specialty patterns. We evaluated differences in outcomes by physician specialty patterns using analysis of variance (ANOVA) and Pearson's chi-square tests (P < .05, two-tailed).
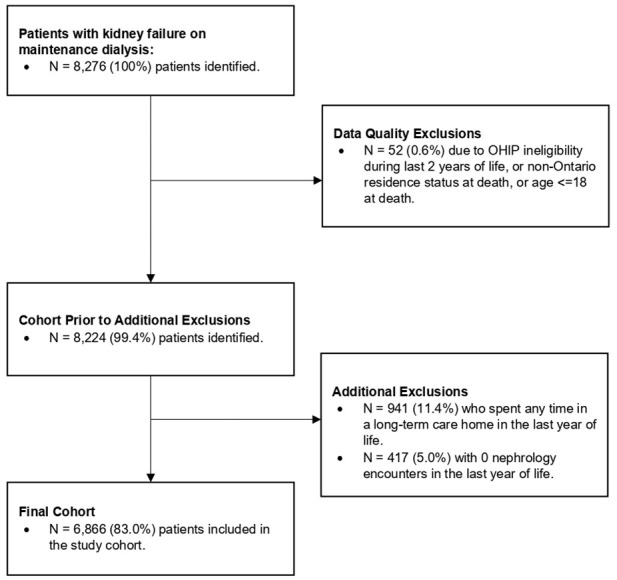
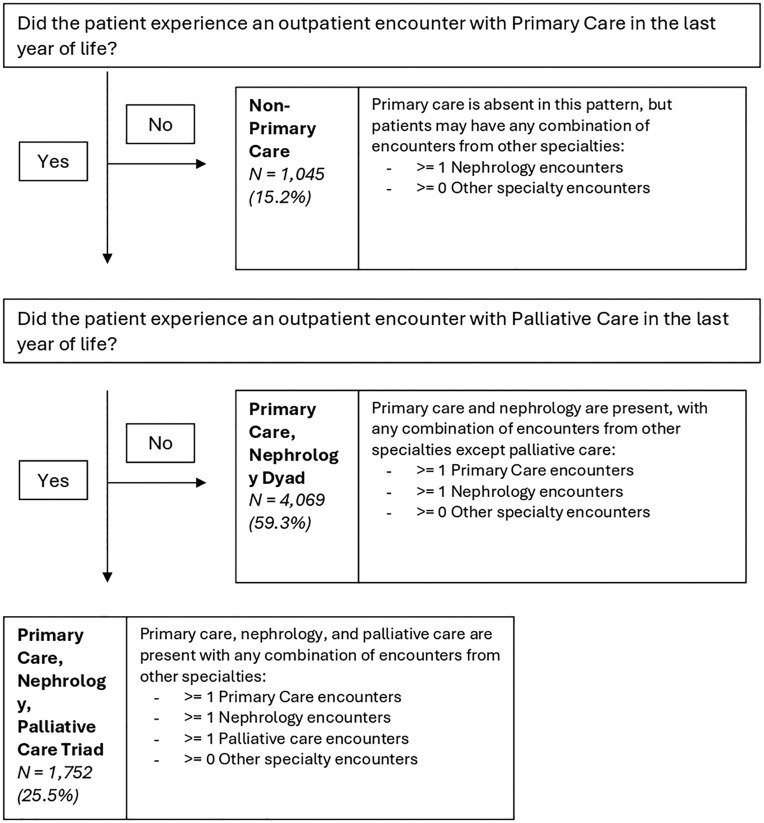
Results: Among 6866 patients, the median age at death was 73, 36.1% were female, and 87.8% resided in urban regions. Three patterns emerged: a primary care, nephrology, and palliative care triad (25.5%); a primary care and nephrology dyad (59.3%); and a non-primary care pattern (15.2%). Palliative care involvement is concentrated near death. Of all, 81.4% spent at least 1 day in hospital or emergency department in the last month, but those with primary care, palliative care, and nephrology involvement had the fewest acute care deaths (65.8%).
Limitations: Outpatient care patterns were defined using physician billing codes, potentially missing care from other providers.
Conclusions: Nephrology and primary care predominantly manage outpatient care in the last year of life for patients with KF on maintenance dialysis, with consistent acute care use across care patterns except for the place of death. Future research should explore associations between patterns of care and end-of-life outcomes to identify the most optimal model of care for patients with KF on maintenance dialysis.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


