Sindhu Sree Rallapalli, Murali Rayani, George Abraham Ninan, Mohammed Anwar Hussain, Aditya V. Nair, Deepti Bal, Kripa Elizabeth Cherian, A. T. Prabhakar, Thomas V. Paul, Nihal Thomas
{"title":"Posterior reversible encephalopathy syndrome and parkinsonism as the first manifestation of primary hyperparathyroidism - a report of two cases","authors":"Sindhu Sree Rallapalli, Murali Rayani, George Abraham Ninan, Mohammed Anwar Hussain, Aditya V. Nair, Deepti Bal, Kripa Elizabeth Cherian, A. T. Prabhakar, Thomas V. Paul, Nihal Thomas","doi":"10.1007/s12020-024-04041-6","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background/objective</h3><p>Primary hyperparathyroidism (PHPT) may be asymptomatic or present with renal calculi, secondary osteoporosis, fractures and neuropsychiatric manifestations. Posterior reversible encephalopathy syndrome (PRES) and parkinsonism are atypical manifestations that may be rarely associated with PHPT. We report two patients who presented with the conditions mentioned above.</p><h3 data-test=\"abstract-sub-heading\">Case report</h3><p>The first patient involved a 38-year-old woman who presented with diminution of vision, seizures, altered behavior and hypertension over eight months. An MRI of the brain done had shown vasogenic edema involving the parieto-occipital regions, suggestive of PRES. A metabolic screen revealed PTH-dependent hypercalcemia that was localized to the left inferior parathyroid gland. Following focused parathyroidectomy, there was improvement in sensorium, vision and normalization of blood pressure. The second patient was of a 74-year-old man who presented with progressive extrapyramidal symptoms of gait abnormalities and rigidity since the past eight months. He was initiated on Selegeline and Levodopa for the same purpose, and subsequently reported minimal improvement in symptoms. Investigations revealed PHPT associated with a right inferior parathyroid adenoma. Within two weeks following surgery, there was an improvement in rigidity and gait and he was able to ambulate without support.</p><h3 data-test=\"abstract-sub-heading\">Discussion</h3><p>PRES has been reported to occur in the context of preeclampsia, hypertension, infection, sepsis and autoimmune conditions. PRES associated with hypercalcemia is rarely reported. While extra-pyramidally related manifestations are described in hypoparathyroidism, PHPT related parkinsonism is not commonly encountered. Identifying the underlying aetiology and initiation of corrective measures may lead to amelioration of patient symptomatology.</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>The occurrence of PRES and parkinsonism is rare in primary hyperparathyroidism; the two patients described above highlight the importance of screening for hypercalcemia in the setting of neurological manifestations.</p>","PeriodicalId":11572,"journal":{"name":"Endocrine","volume":"7 1","pages":""},"PeriodicalIF":3.7000,"publicationDate":"2024-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12020-024-04041-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background/objective
Primary hyperparathyroidism (PHPT) may be asymptomatic or present with renal calculi, secondary osteoporosis, fractures and neuropsychiatric manifestations. Posterior reversible encephalopathy syndrome (PRES) and parkinsonism are atypical manifestations that may be rarely associated with PHPT. We report two patients who presented with the conditions mentioned above.
Case report
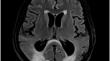
The first patient involved a 38-year-old woman who presented with diminution of vision, seizures, altered behavior and hypertension over eight months. An MRI of the brain done had shown vasogenic edema involving the parieto-occipital regions, suggestive of PRES. A metabolic screen revealed PTH-dependent hypercalcemia that was localized to the left inferior parathyroid gland. Following focused parathyroidectomy, there was improvement in sensorium, vision and normalization of blood pressure. The second patient was of a 74-year-old man who presented with progressive extrapyramidal symptoms of gait abnormalities and rigidity since the past eight months. He was initiated on Selegeline and Levodopa for the same purpose, and subsequently reported minimal improvement in symptoms. Investigations revealed PHPT associated with a right inferior parathyroid adenoma. Within two weeks following surgery, there was an improvement in rigidity and gait and he was able to ambulate without support.
Discussion
PRES has been reported to occur in the context of preeclampsia, hypertension, infection, sepsis and autoimmune conditions. PRES associated with hypercalcemia is rarely reported. While extra-pyramidally related manifestations are described in hypoparathyroidism, PHPT related parkinsonism is not commonly encountered. Identifying the underlying aetiology and initiation of corrective measures may lead to amelioration of patient symptomatology.
Conclusion
The occurrence of PRES and parkinsonism is rare in primary hyperparathyroidism; the two patients described above highlight the importance of screening for hypercalcemia in the setting of neurological manifestations.
期刊介绍:
Well-established as a major journal in today’s rapidly advancing experimental and clinical research areas, Endocrine publishes original articles devoted to basic (including molecular, cellular and physiological studies), translational and clinical research in all the different fields of endocrinology and metabolism. Articles will be accepted based on peer-reviews, priority, and editorial decision. Invited reviews, mini-reviews and viewpoints on relevant pathophysiological and clinical topics, as well as Editorials on articles appearing in the Journal, are published. Unsolicited Editorials will be evaluated by the editorial team. Outcomes of scientific meetings, as well as guidelines and position statements, may be submitted. The Journal also considers special feature articles in the field of endocrine genetics and epigenetics, as well as articles devoted to novel methods and techniques in endocrinology.
Endocrine covers controversial, clinical endocrine issues. Meta-analyses on endocrine and metabolic topics are also accepted. Descriptions of single clinical cases and/or small patients studies are not published unless of exceptional interest. However, reports of novel imaging studies and endocrine side effects in single patients may be considered. Research letters and letters to the editor related or unrelated to recently published articles can be submitted.
Endocrine covers leading topics in endocrinology such as neuroendocrinology, pituitary and hypothalamic peptides, thyroid physiological and clinical aspects, bone and mineral metabolism and osteoporosis, obesity, lipid and energy metabolism and food intake control, insulin, Type 1 and Type 2 diabetes, hormones of male and female reproduction, adrenal diseases pediatric and geriatric endocrinology, endocrine hypertension and endocrine oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


