Aortic isthmus flow reversal in fetal coarctation of the aorta and the associated factors
Abstract
Introduction
The aim of this study was to investigate the presence of aortic isthmus flow reversal and its associated factors in fetuses with positive and false-positive coarctation of the aorta (CoA) compared with normal controls.
Material and Methods
Pregnant women with fetuses suspected of CoA and normal control were enrolled, and these women experienced prenatal ultrasound scan and followed up for 6 months after birth to confirm the presence of CoA. All the ultrasound parameters were analyzed.
Results
A total of 134 pregnant women were enrolled, with 43 CoA-positive fetuses and 91 CoA false-positive fetuses, and 334 matched pregnant women were enrolled in the control group. Aortic isthmus flow reversal occurred in 28 (65.1%) fetuses in the CoA-positive group, significantly (p < 0.05) more than in the false-positive (37 or 40.7%) or control group (64 or 19.2%). Aortic isthmus flow reversal was mostly in the full systole (n = 17 or 60.7%) or late systole and early-middle diastole (n = 10 or 35.7%) in the CoA-positive fetuses (n = 27 or 96.4%), significantly (p < 0.001) different from that in the false-positive or control group. The aortic isthmus flow reversal peak systolic velocity (PSV), flow volume, and ratio of reversed flow/forward flow were significantly (p < 0.05) increased in the CoA-positive and false-positive groups than in the control group. The aortic isthmus flow reversal incidence was significantly (p < 0.05) correlated with the middle cerebral artery (MCA) PSV in the total three groups or in the false-positive group but was significantly (p < 0001) negatively correlated with the MCA resistance index (RI) in the CoA-positive group. The incidence of the aortic isthmus flow reversal was significantly (p < 0.05) positively correlated with the umbilical artery (UA) RI in the false-positive group and with the UA RI in the total three groups. Independently associated factors for aortic isthmus flow reversal were isthmic flow volume/CCO (combined cardiac output) in the CoA-positive group.
Conclusions
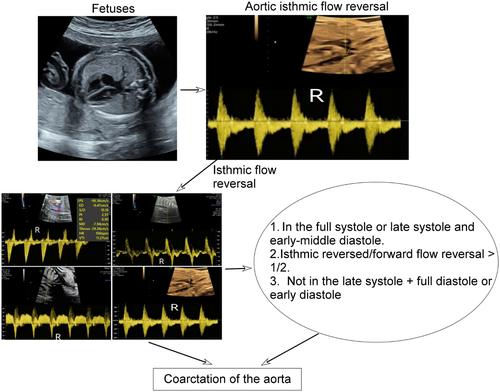
Reversal of flow in the aortic isthmus is much more common in true-positive cases of CoA as compared to controls, and isthmic flow reversal in the full systolic phase only suggests presence of CoA. The aortic isthmic reversed flow volume accounts for over half of the isthmic forward flow volume in the CoA-positive fetuses than in the normal controls.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


