Impact of Different Angiotensin-Converting Enzyme Inhibitors or Angiotensin Receptor Blocker Resumption Timing on Post Acute Kidney Injury Outcomes
IF 5.7
2区 医学
Q1 UROLOGY & NEPHROLOGY
引用次数: 0
Abstract
Introduction
Evidence suggests a survival benefit from resuming angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB) post acute kidney injury (AKI) compared to nonuse; however, the optimal timing and its impact on outcomes are unclear. The risks of earlier resumption, such as recurrent AKI or hyperkalemia, remain unexplored.
Methods
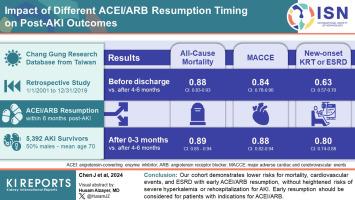
Using multiinstitutional electronic health records, we analyzed the relationship between 3 ACEI or ARB (ACEI/ARB) resumption timelines post-AKI (prior to discharge, 0–3 months, and 4–6 months postdischarge) and outcomes including all-cause mortality, major adverse cardiac and cerebrovascular events (MACCEs), dialysis initiation or end-stage renal disease (ESRD), severe hyperkalemia, and recurrent AKI with hospitalization. Cox proportional models estimated hazard ratios (HRs) for outcomes across different resumption timings, following a target trial design.
Results
Among 5392 AKI survivors resuming ACEI/ARB within 6 months post-AKI, earlier resumption was associated with lower mortality, MACCE, MACCE-related mortality, new dialysis initiation or ESRD (P < 0.001 in trend tests), without increased risks of severe hyperkalemia and re-AKI admissions. Early resumption has a lower mortality compared to 4 to 6 months postdischarge (before discharge, HR: 0.88, 95% confidence interval [CI]: 0.83–0.93; 0–3 months, HR: 0.89, 95% CI: 0.85–0.94). Subgroup analysis showed a lower mortality HR from earlier resumption among AKI survivors with prior ACEI/ARB comorbidity indications (P < 0.001 in trend tests; before discharge, HR: 0.85, 95% CI: 0.80–0.90; 0–3 months, HR: 0.88, 95% CI: 0.83–0.93).
Conclusion
Our cohort demonstrates lower risks for mortality, cardiovascular events, and ESRD with early ACEI/ARB resumption, without heightened risks of severe hyperkalemia or rehospitalization for AKI. Early resumption should be considered for patients with indications for ACEI/ARB.
不同的血管紧张素转换酶抑制剂或血管紧张素受体阻滞剂恢复使用时间对急性肾损伤后结果的影响
有证据表明,与不使用血管紧张素转换酶抑制剂(ACEI)或血管紧张素受体阻滞剂(ARB)相比,急性肾损伤(AKI)后恢复使用血管紧张素转换酶抑制剂(ACEI)或血管紧张素受体阻滞剂(ARB)对患者的生存有益;然而,最佳时机及其对预后的影响尚不清楚。提前恢复用药的风险(如复发性 AKI 或高钾血症)仍未得到探讨。利用多机构电子健康记录,我们分析了 AKI 后 3 个 ACEI 或 ARB(ACEI/ARB)恢复时间(出院前、出院后 0-3 个月和出院后 4-6 个月)与全因死亡率、主要不良心脑血管事件 (MACCE)、开始透析或终末期肾病 (ESRD)、严重高钾血症和复发性 AKI 与住院之间的关系。根据目标试验设计,Cox 比例模型估算了不同恢复时间的结果危险比 (HR)。在 AKI 后 6 个月内恢复 ACEI/ARB 的 5392 名 AKI 幸存者中,较早恢复与较低的死亡率、MACCE、MACCE 相关死亡率、新的透析启动或 ESRD 相关(趋势检验 <0.001),但不会增加严重高钾血症和再次 AKI 住院的风险。与出院后 4-6 个月相比,早期恢复透析的死亡率较低(出院前,HR:0.88,95% 置信区间 [CI]:0.83-0.93;出院后,HR:0.88-0.93,95% 置信区间 [CI]:0.83-0.93):0.83-0.93;0-3 个月,HR:0.89,95% 置信区间 [CI]:0.85-0.94)。亚组分析表明,在既往有 ACEI/ARB 并发症指征的 AKI 幸存者中,较早恢复治疗的死亡率 HR 更低(趋势检验 <0.001;出院前,HR:0.85,95% CI:0.80-0.90;0-3 个月,HR:0.88,95% CI:0.83-0.93)。我们的队列显示,早期恢复 ACEI/ARB 可降低死亡率、心血管事件和 ESRD 风险,但不会增加严重高钾血症或因 AKI 再次住院的风险。有 ACEI/ARB 适应症的患者应考虑尽早恢复治疗。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Kidney International Reports
Medicine-Nephrology
CiteScore
7.70
自引率
3.30%
发文量
1578
审稿时长
8 weeks
期刊介绍:
Kidney International Reports, an official journal of the International Society of Nephrology, is a peer-reviewed, open access journal devoted to the publication of leading research and developments related to kidney disease. With the primary aim of contributing to improved care of patients with kidney disease, the journal will publish original clinical and select translational articles and educational content related to the pathogenesis, evaluation and management of acute and chronic kidney disease, end stage renal disease (including transplantation), acid-base, fluid and electrolyte disturbances and hypertension. Of particular interest are submissions related to clinical trials, epidemiology, systematic reviews (including meta-analyses) and outcomes research. The journal will also provide a platform for wider dissemination of national and regional guidelines as well as consensus meeting reports.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


